Case 9 - A 46 y.o. LADY
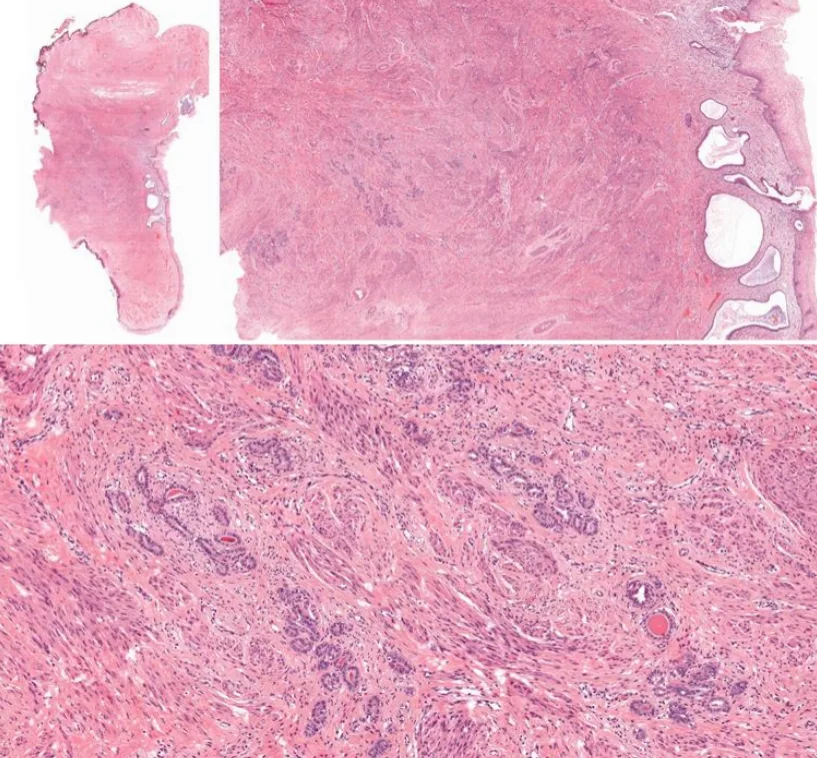
was diagnosed with adenocarcinoma in situ on pap smear and she underwent cervical cone biopsy. One representative section.
🎯𝘛𝘈𝘙𝘎𝘌𝘛𝘌𝘋 𝘋𝘐𝘈𝘎𝘕𝘖𝘚𝘐𝘚 🎯
- Published on
Granular cell tumors were described as early as 1926 by the Russian pathologist Abrikossoff. They were initially coined granular cell myoblastomas, as they were believed to be of muscular origin. With the advent of immunohistochemical stains and electron microscopy, they are now believed to be Schwannian derivation. Notably, a subset of S100-negative “non-neural” granular cell tumors have been identified which may not derive from neural tissue.
These rare tumors are most commonly reported in the skin, oral cavity, digestive tract, and subcutaneous tissue. However, they can occur anywhere in the body, including breast, bladder, nervous system, respiratory and genitourinary tracts. All age groups and genders can be affected, but it is classically found in women in their 4th to 6th decades of life.Granular cell tumors typically present as solitary, painless nodules less than 3-4 cm large and may be found incidentally.
The vast majority behave indolently. Based on histologic criteria or the presence of metastasis, however, 1% to 2% of these lesions can be malignant, with poor prognosis and few curative options beyond surgical excision.
These rare tumors are most commonly reported in the skin, oral cavity, digestive tract, and subcutaneous tissue. However, they can occur anywhere in the body, including breast, bladder, nervous system, respiratory and genitourinary tracts. All age groups and genders can be affected, but it is classically found in women in their 4th to 6th decades of life.Granular cell tumors typically present as solitary, painless nodules less than 3-4 cm large and may be found incidentally.
The vast majority behave indolently. Based on histologic criteria or the presence of metastasis, however, 1% to 2% of these lesions can be malignant, with poor prognosis and few curative options beyond surgical excision.
17 years old girl with no known medical illness. C/o swelling over left middle finger for past 1 year. Gradually increasing in size. Pain when pressured eg. picking up object. No limited range of movement. Clinical dx: Left middle finger giant cell tumour (volar)
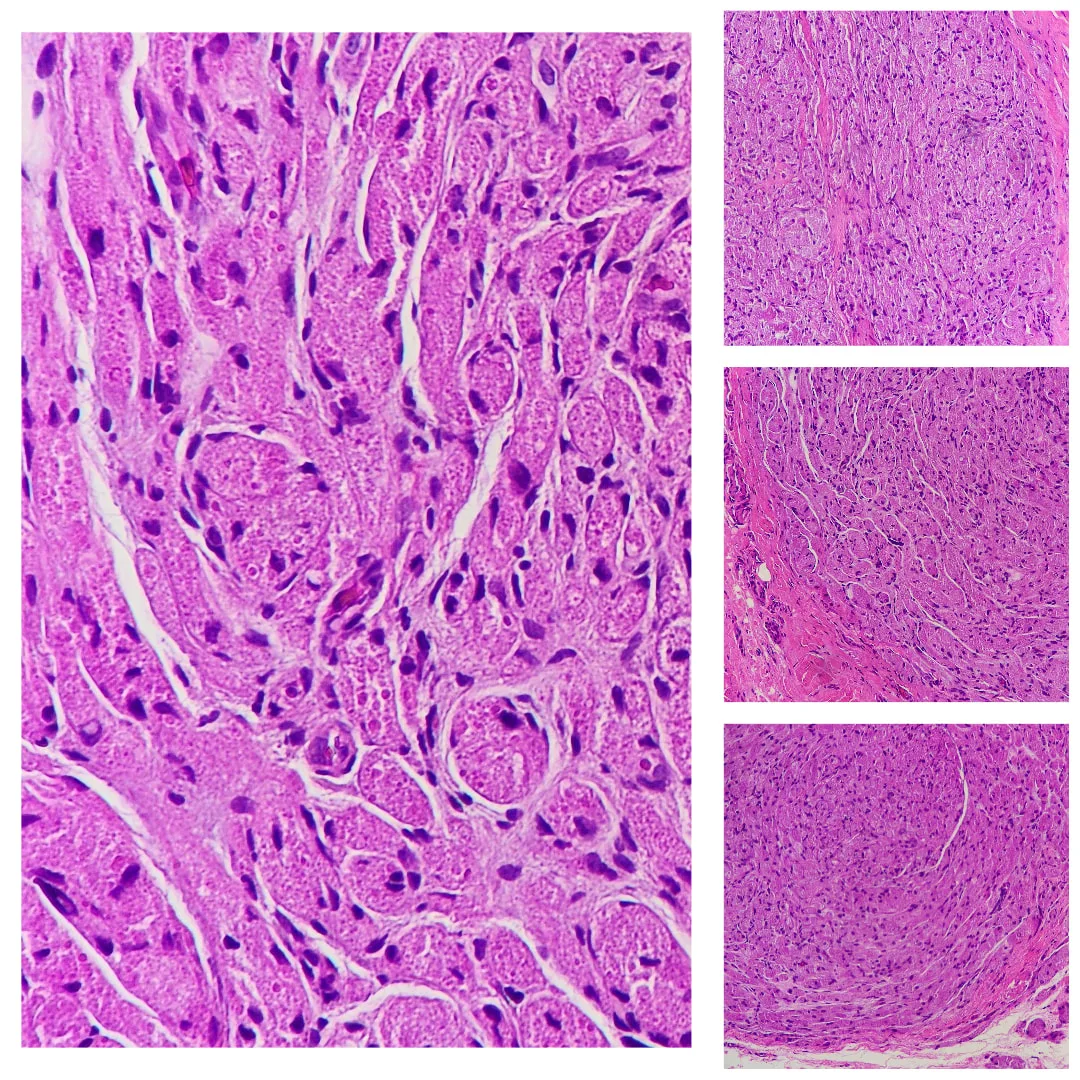
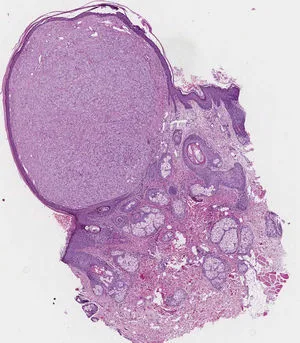
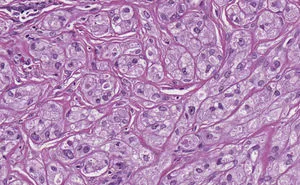
In granular cell tumour, sections show broad fascicles of tumour cells arranged in nests or sheets infiltrating the dermis and dermal structures. The tumour cells are large in size, with small, uniform, eosinophilic granules filling the cytoplasm, and small, round-to-oval nuclei. Mitoses are rare.
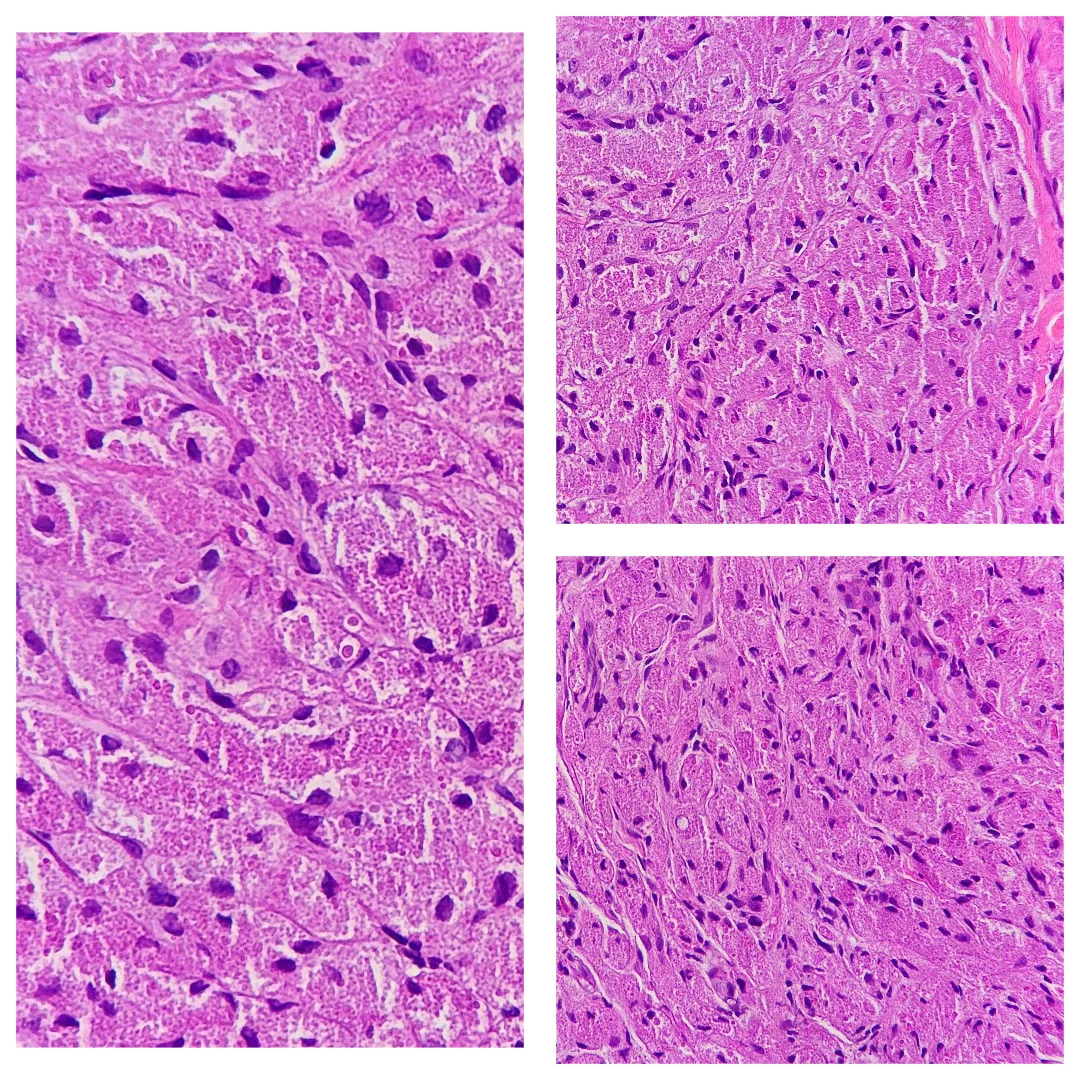
'Pustulo-ovoid bodies of Milian' may be present. These are large granules surrounded by a clear halo.
Sections show broad fascicles of tumour cells arranged in nests or sheets infiltrating the dermis and dermal structures.
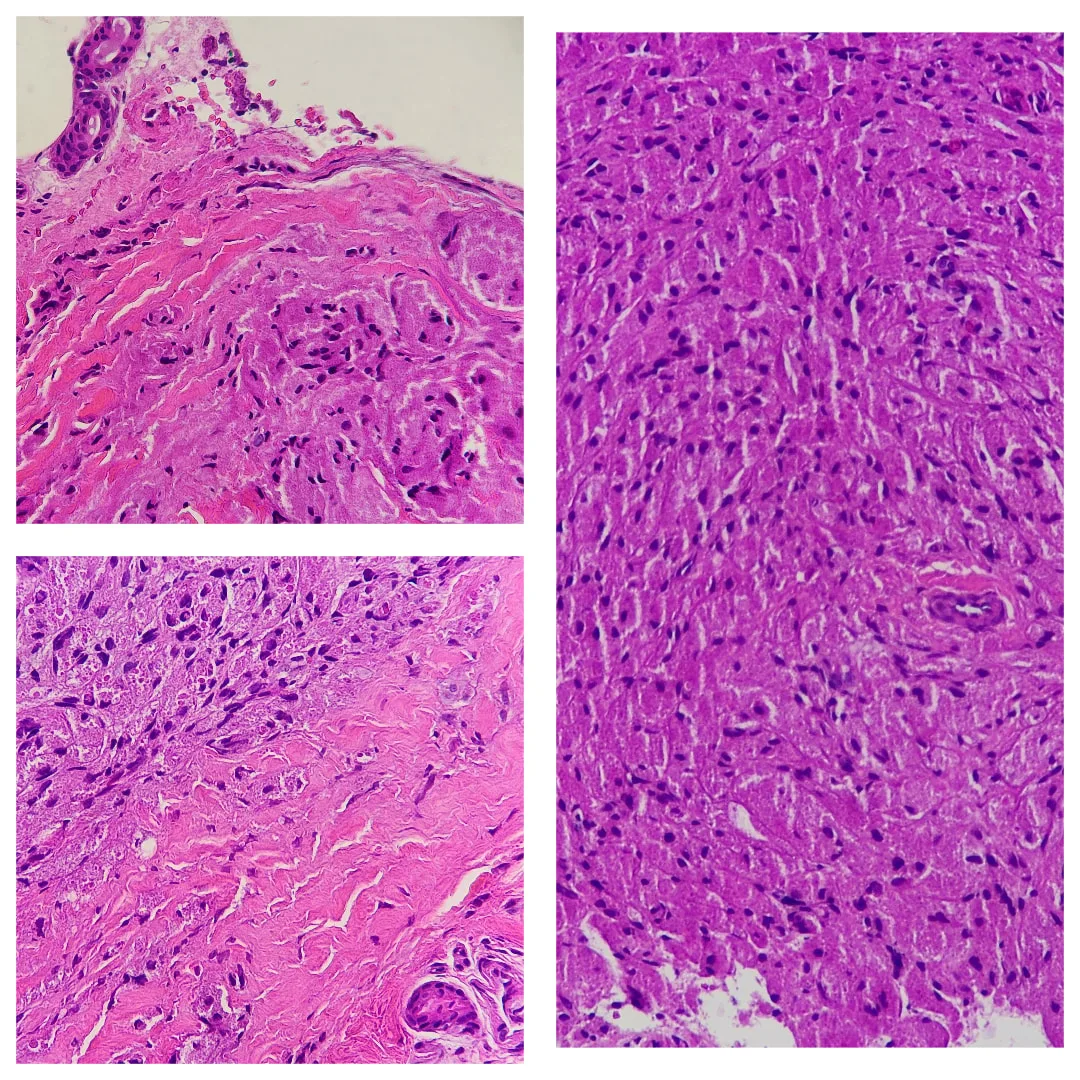
Sometimes, the overlying epidermis may become markedly hyperplastic and mimic a squamous cell carcinoma. This is thought to be a reactive phenomenon.
Malignant forms of granular cell tumour are extremely rare but reported. Frank anaplasia, increased mitotic activity and tumour necrosis are worrisome features.
Sometimes, the overlying epidermis may become markedly hyperplastic and mimic a squamous cell carcinoma. This is thought to be a reactive phenomenon.
Malignant forms of granular cell tumour are extremely rare but reported. Frank anaplasia, increased mitotic activity and tumour necrosis are worrisome features.
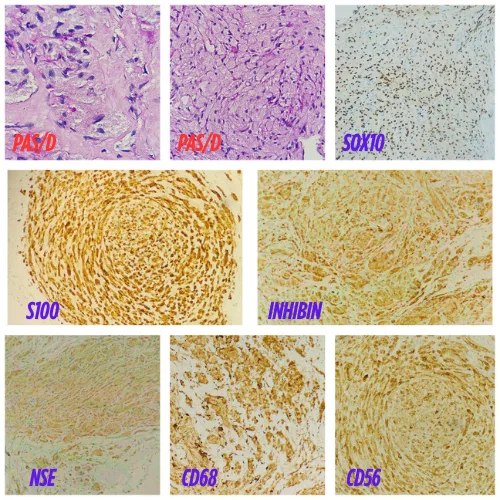
Special studies for granular cell tumour
S-100 protein is positive. PAS highlights granules after diastase digestion. Other positive stains may include SOX10 , inhibin , neuron specific enolase, CD68, and CD56.
Differential diagnosis of granular cell tumour pathology :
Rhabdomyoma — These may be similar to granular cell tumour. Rhabdomyomas are positive with desmin and myoglobin.
S-100 immunohistochemical positivity in rhabdomyoma: An underestimated potential diagnostic pitfall in routine practice
Gingival granular cell tumour of newborn ( Congenital epulis of newborn)— These are morphologically similar to granular cell tumour but arise in a distinct clinical setting. S100 is negative.
Other tumours with granular cells – Granular cell change has been described in many other tumours (including dermatofibroma, fibrous papule, AFX and primitive polypoid granular cell tumour - See below). S100 positivity is generally a useful diagnostic aid.
S-100 protein is positive. PAS highlights granules after diastase digestion. Other positive stains may include SOX10 , inhibin , neuron specific enolase, CD68, and CD56.
Differential diagnosis of granular cell tumour pathology :
Rhabdomyoma — These may be similar to granular cell tumour. Rhabdomyomas are positive with desmin and myoglobin.
S-100 immunohistochemical positivity in rhabdomyoma: An underestimated potential diagnostic pitfall in routine practice
Gingival granular cell tumour of newborn ( Congenital epulis of newborn)— These are morphologically similar to granular cell tumour but arise in a distinct clinical setting. S100 is negative.
Other tumours with granular cells – Granular cell change has been described in many other tumours (including dermatofibroma, fibrous papule, AFX and primitive polypoid granular cell tumour - See below). S100 positivity is generally a useful diagnostic aid.
Primitive Polypoid Granular-Cell Tumor
Tumor in the superficial and mid dermis, surrounded by an epithelial collarette.
Cells with a polygonal morphology, abundant granular eosinophilic cytoplasm, and large vesicular nuclei. The cells are arranged in an interlinked fascicular pattern.
In contrast to conventional granular cell tumor (Abrikossoff tumor), primitive polypoid granular cell tumor was first identified by LeBoit et al.1 in 1991 and subsequently endorsed by Chaudhry and Calonje2 as a dermal tumor of granular cells of non-neural origin. The tumor has a polypoid morphology and presents numerous mitoses, cytologic atypia, and a primitive immunophenotype.
0 Comments