Case 9 - A 46 y.o. LADY
🎯𝘛𝘈𝘙𝘎𝘌𝘛𝘌𝘋 𝘋𝘐𝘈𝘎𝘕𝘖𝘚𝘐𝘚 🎯
- Published on
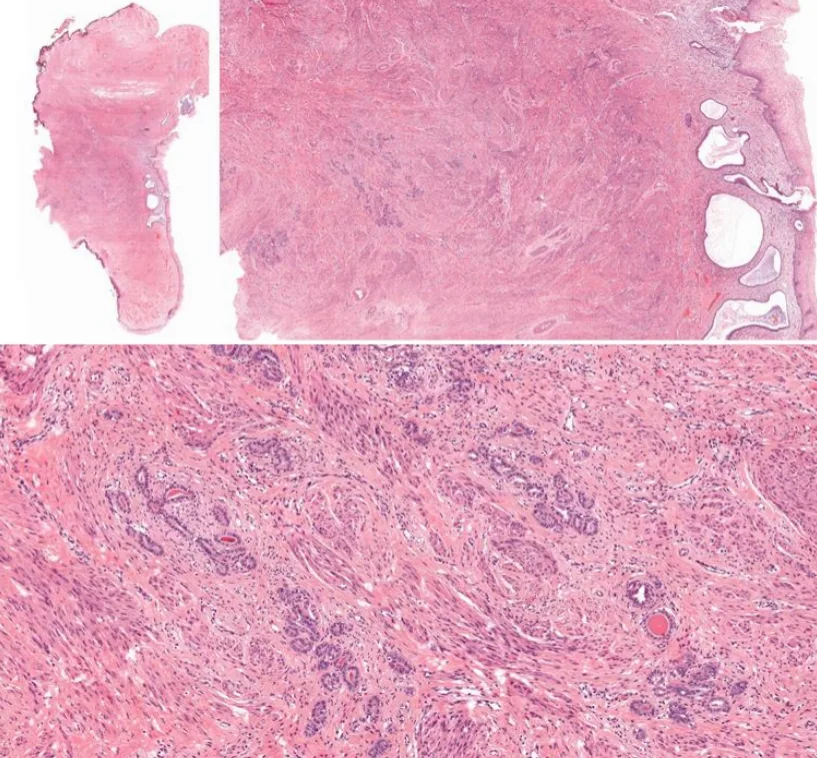
A 46-year-old lady was diagnosed with adenocarcinoma in situ on pap smear and she underwent cervical cone biopsy. One representative section.
Reference 1. Zaino, R. Glandular Lesions of the Uterine Cervix. Mod Pathol 13, 261–274 (2000).
- Published on
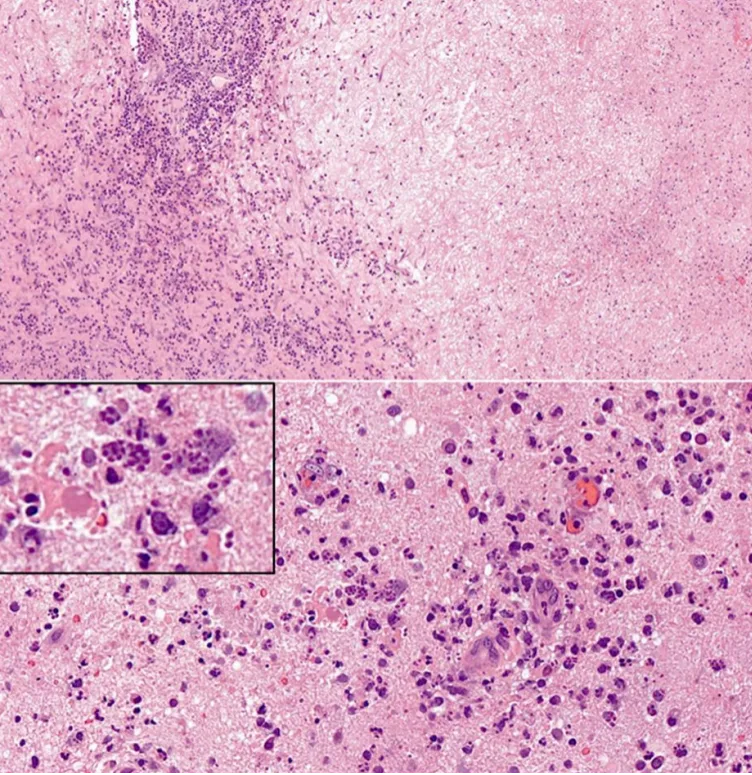
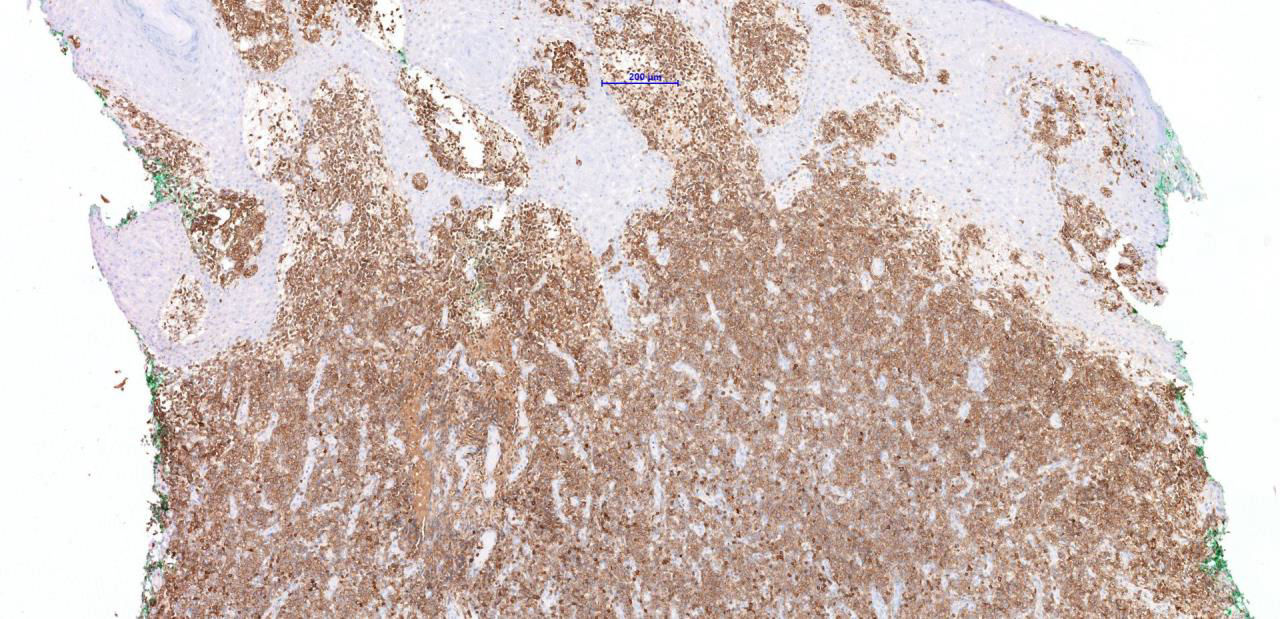
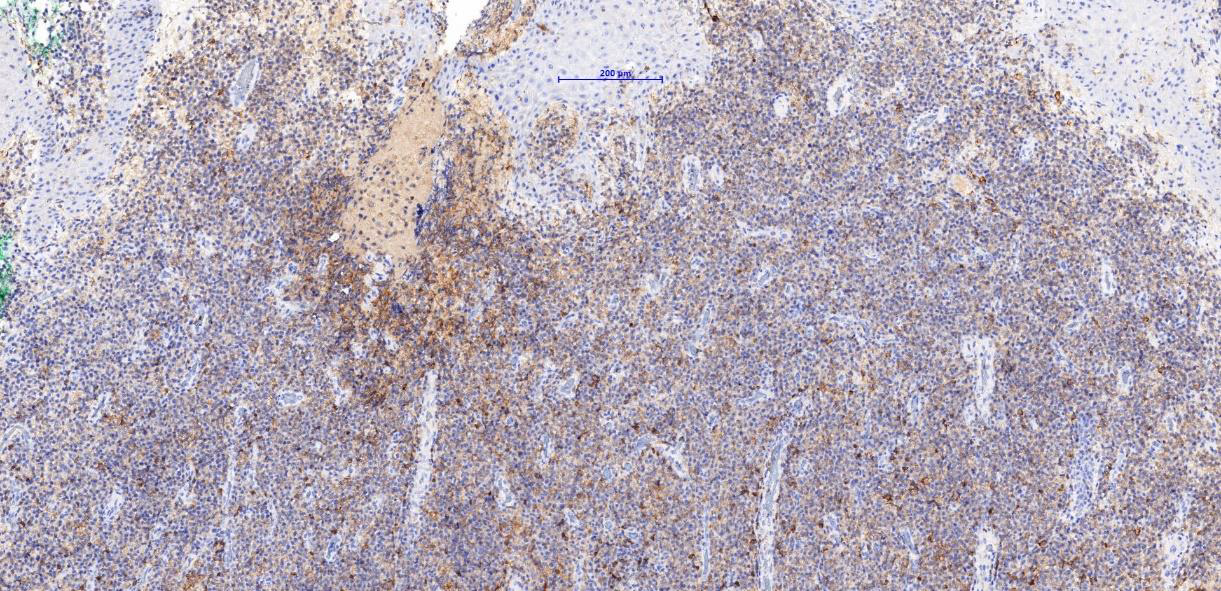
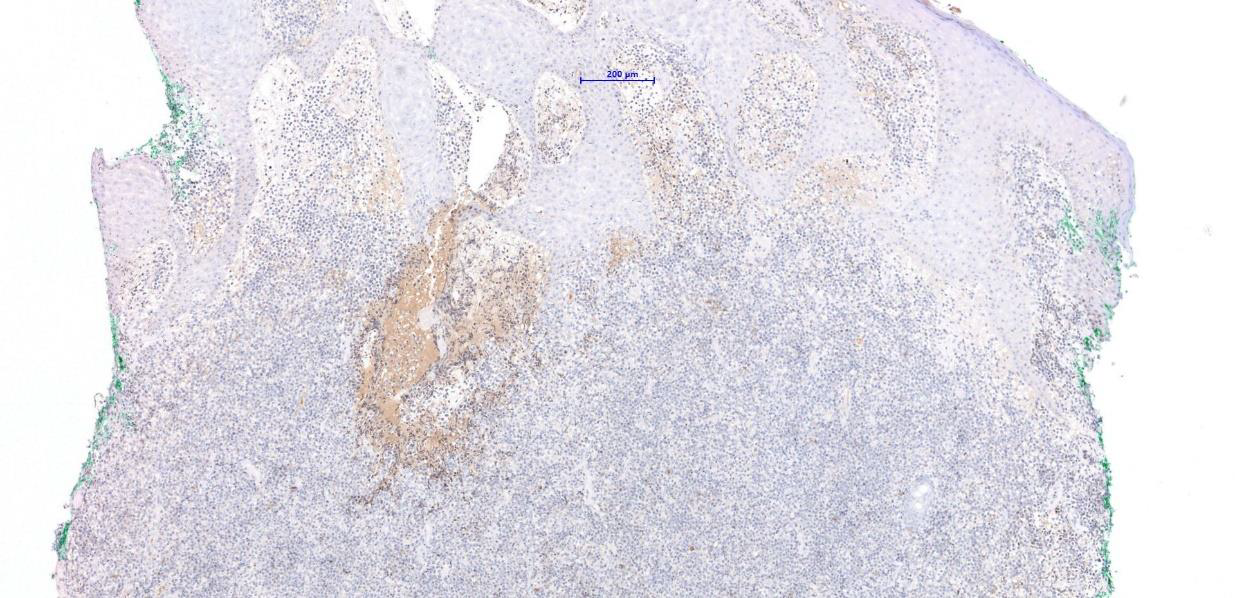
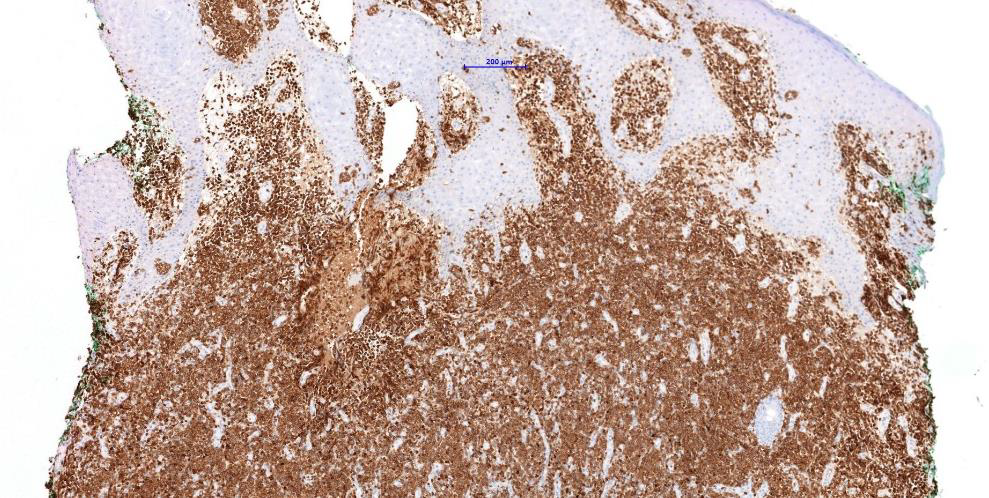
1. The brain tissue fragments show necrotizing cerebritis with large areas of necrosis containing eosinophilic cellular debris. There are foci of mixed acute and chronic inflammatory infiltrates and perivascular inflammatory infiltrates. Extracellular microorganisms and rare pseudocysts are observed, morphologically consistent with free tachyzoites and bradyzoites of Toxoplasma gondii.
2. Most common differential diagnoses for intracranial lesions of AIDS patients are primary central nervous system lymphoma, progressive multifocal leukoencephalopathy, cerebral toxoplasmosis and HIV encephalitis. In this brain tissue biopsy, microorganisms with the size less than a lymphocyte are identified. Histoplasma capsulatum and Toxoplasma gondii are the main differentials. Morphologically, the former is distinguished from the latter by presence of fungal cell wall in the form of halo in H&E stain. This could be highlighted by GMS and PAS special stains. Toxoplasma gondii may be difficult to be recognized due to resemblance to cellular debris. Immunohistochemistry against Toxoplasma gondii is helpful.
Reference 1. Lee, Ashley M., et al. "Safety and diagnostic value of brain biopsy in HIV patients: a case series and metaanalysis of 1209 patients." Journal of Neurology, Neurosurgery & Psychiatry 87.7 (2016): 722-733. 2. Kradin, Richard L. Diagnostic Pathology of Infectious Disease. Elsevier Health Sciences, 2017.
- Published on
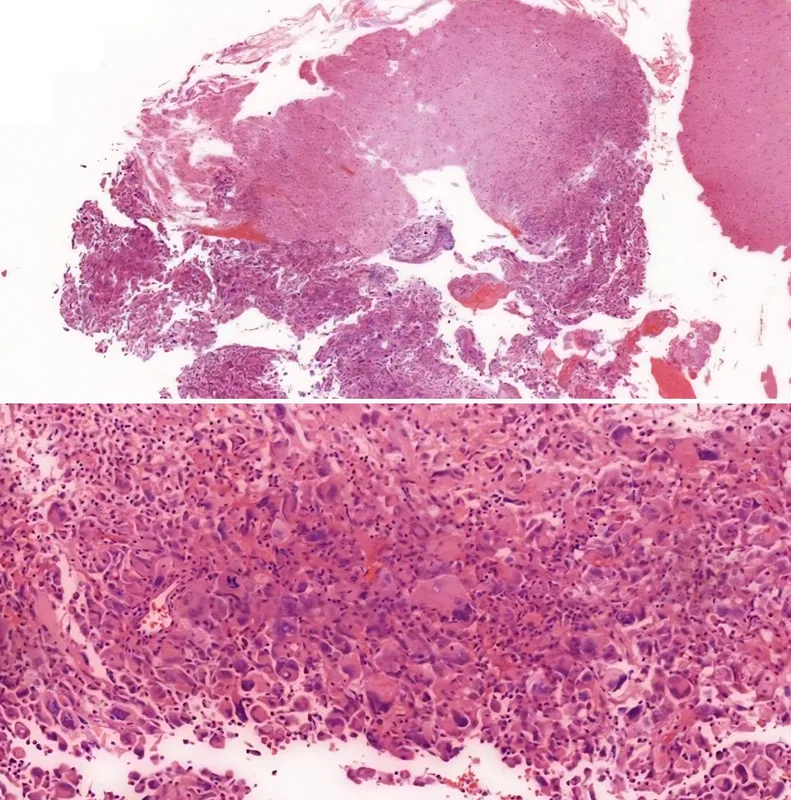
32 y.o., female, multiple hyperdense lesions on the right parietal region. One representative section.Immunohistochemistry shows the malignant cells are positive for GFAP and negative for pan-cytokeratin and HMB-45.
1. Section shows tumor tissue fragments composed of bizarre malignant cells with angulated hyperchromatic nuclei and abundant cytoplasm. Numerous multinucleated tumor giant cells are admixed. Mitoses are easily observed. The adjacent glial tissue is focally infiltrated by malignant
cells. Immunohistochemistry shows the malignant cells are positive for GFAP and negative for pan-cytokeratin and HMB-45. Histological findings are consistent with giant cell glioblastoma, WHO grade IV. (Note: Without IDH evaluation, a diagnosis of glioblastoma, NOS, is more appropriate, vide infra)
2. The 2016 World Health Organization Classification of Tumors of the Central Nervous System employs integrated phenotypic and genotypic parameters for tumor classification. Glioblastomas are classified into (1) glioblastoma, IDH-wildtype (about 90 %), which corresponds to the clinically defined primary or de novo glioblastoma in older patients; (2) glioblastoma, IDH-mutant (about 10%), which corresponds to secondary glioblastoma with a history of prior lower grade diffuse glioma in younger patients, and (3) glioblastoma, NOS, a diagnosis for those tumors that IDH
evaluation cannot be performed.
3. Along with gliosarcoma and epithelioid glioblastoma, giant cell glioblastoma is a variant under the umbrella of glioblastoma, IDH-wildtype. Histologically, it is characterized by bizarre, multinucleated giant cells and an occasionally abundant reticulin network. Palisading and large
ischaemic necroses are observed. Atypical mitoses are frequent. Microvascular proliferation is not common. Giant cell glioblastoma has a somewhat better prognosis than ordinary glioblastoma.
Reference:
1. World Health Organization. (2016). WHO Classification of Tumours of the Central Nervous System Revised 4th Edition. David N. Louis, (Ed.). Internat. Agency for Research on Cancer.
- Published on
EDUCATIONAL NOTES:
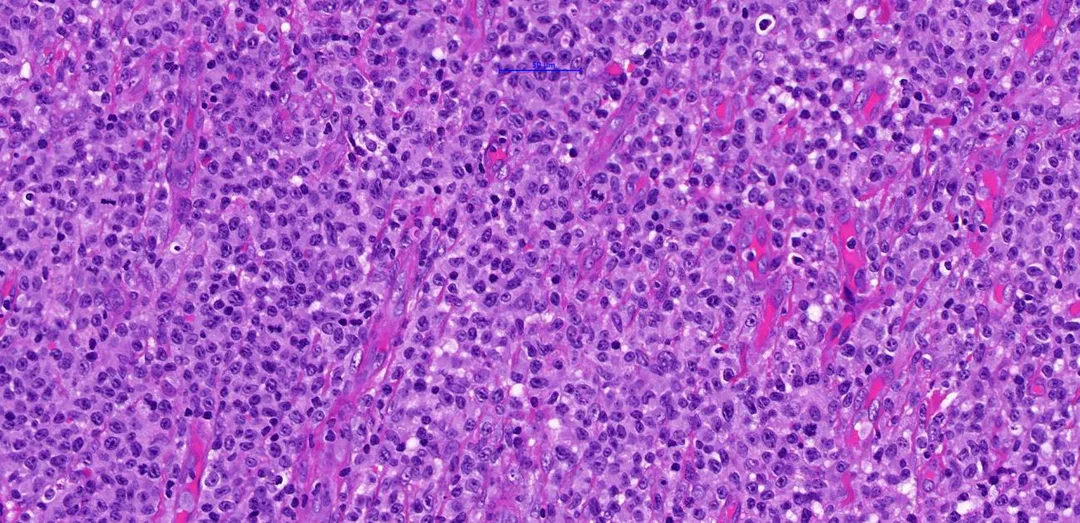
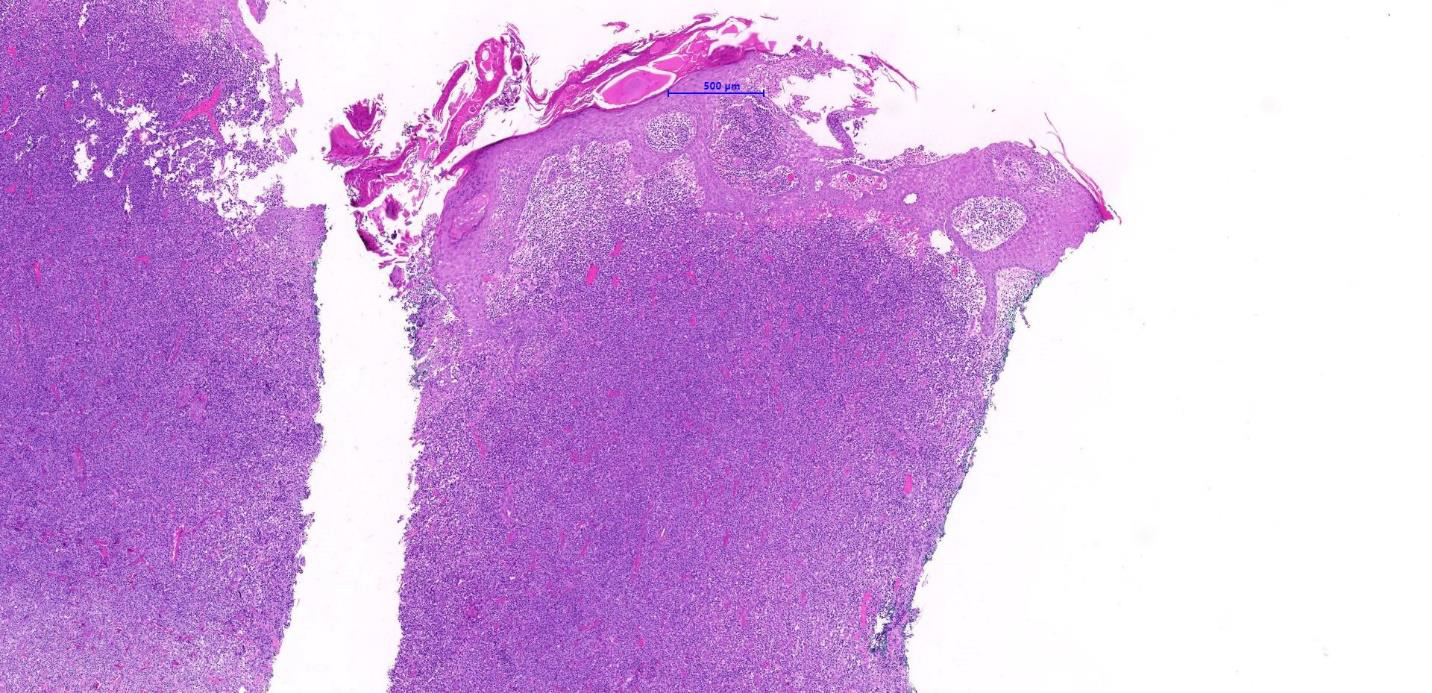
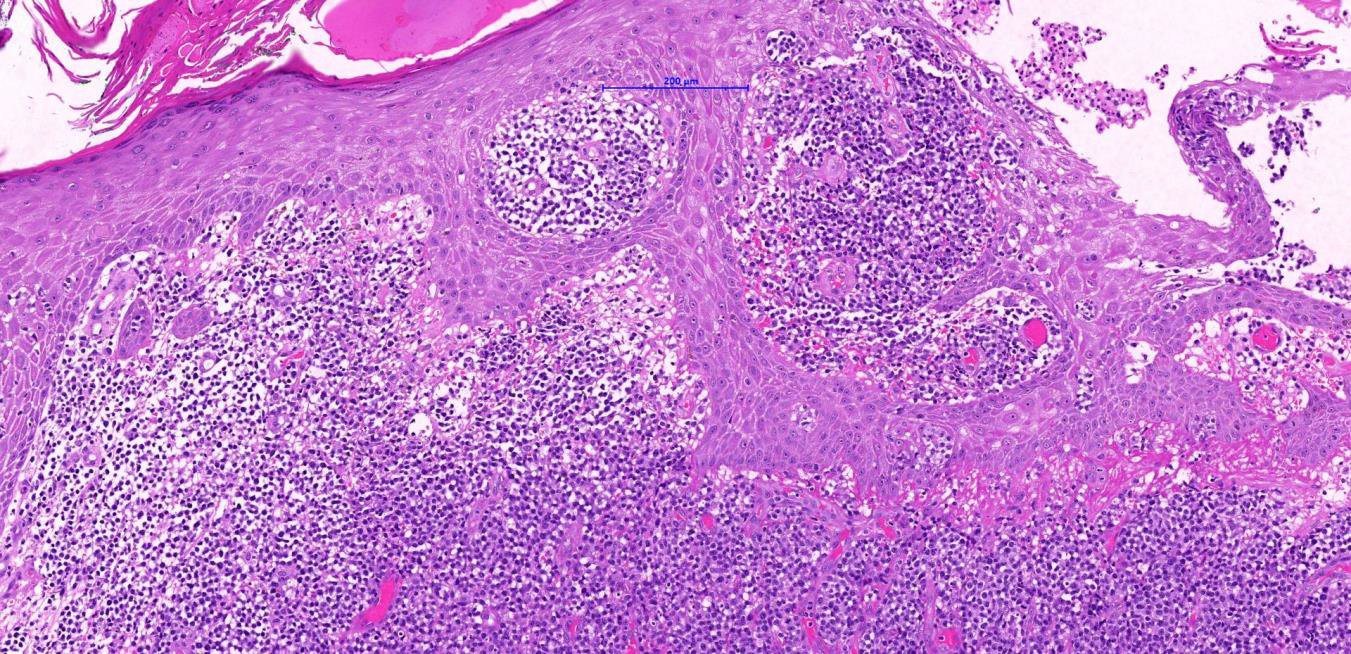
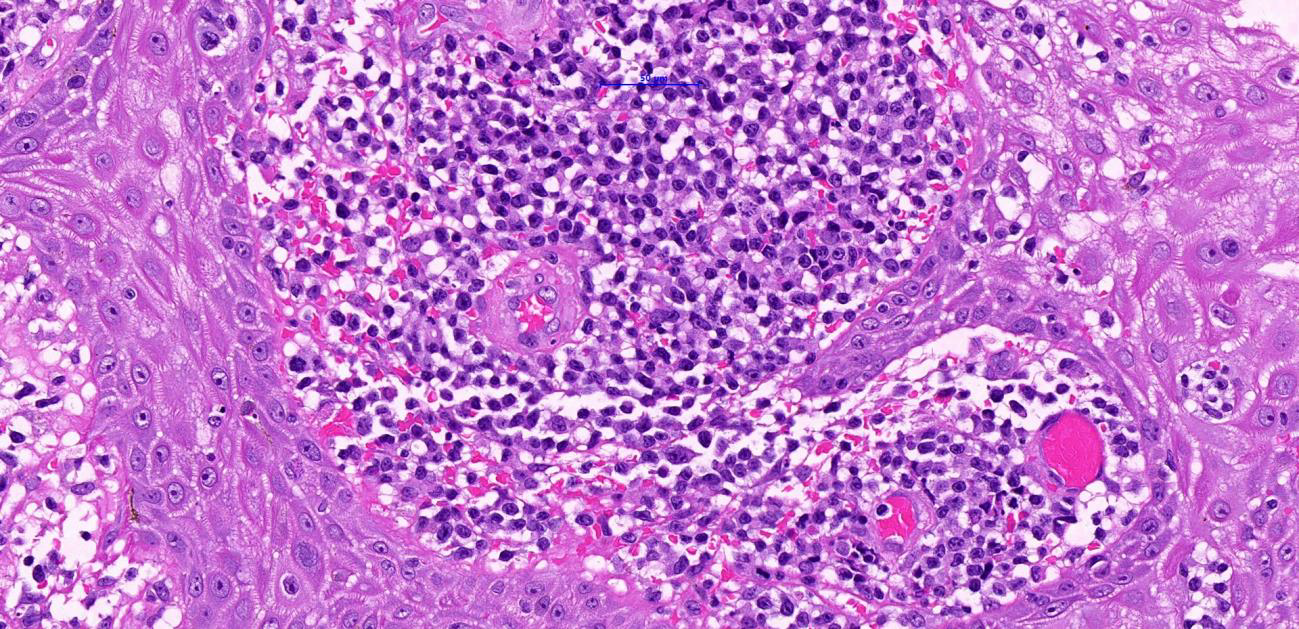
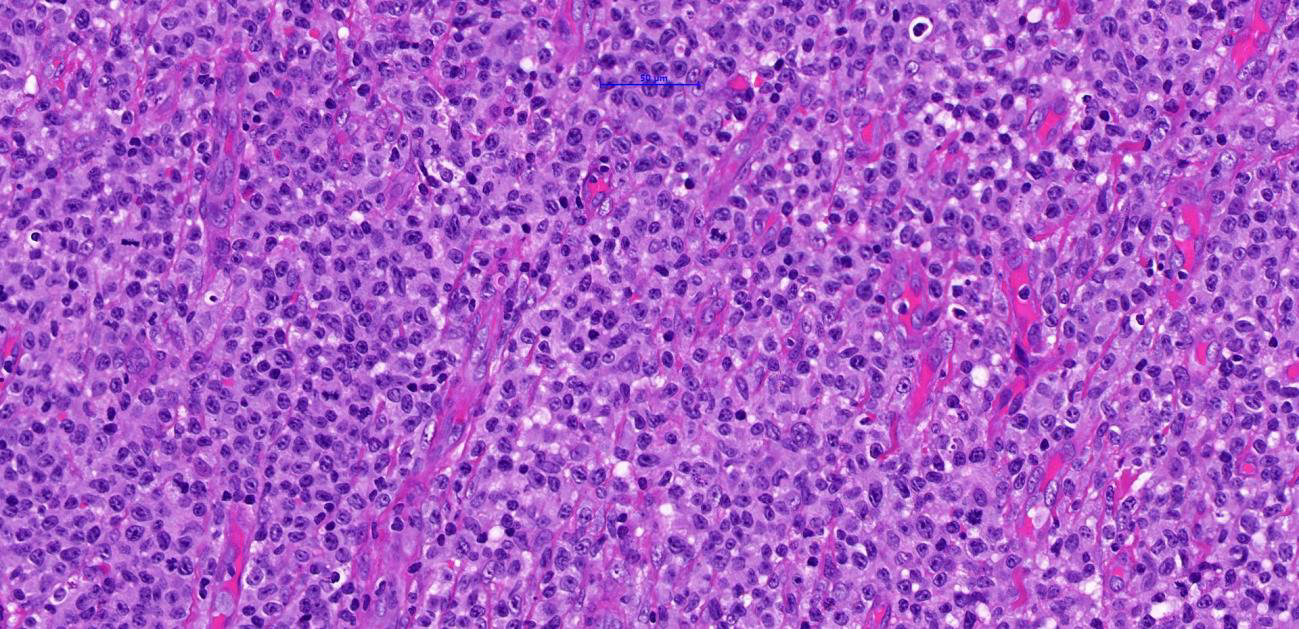
1) Section from the left thigh punch biopsy shows diffuse dermal infiltration by large neoplastic lymphoid cells arranged in solid sheets. The cells display moderate to markedly pleomorphic vesicular nuclei with prominent multiple nucleoli. The cytoplasm is eosinophilic and ample in amount. Mitotic figures are frequently seen.
Occasional histiocytes and small reactive lymphocytes are appreciated in the background.
The overlying epidermis shows marked acanthosis and parakeratosis with prominent lymphocyte epidermotropism and Pautrier microabscesses. No angio-invasion or angio-destruction is seen.
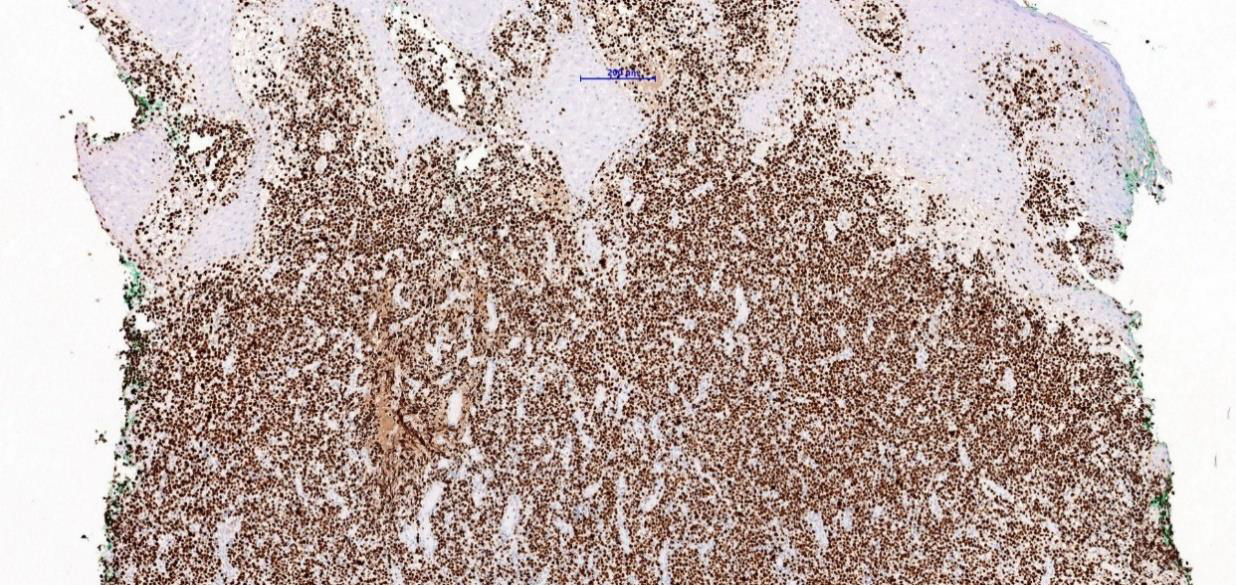
2) Immunohistochemistry study shows the neoplastic lymphoid cells are immunoreactive (+) for CD2, CD3 and CD5, with aberrant loss in CD7 and CD8. CD4 is positive (+) in a significant number of cells. CD30, ALK-1 and CD20 are negative (-). The proliferative index as estimated by Ki67 is high (>90%).
3) The evolution of patches and plaques followed by tumoral stage further supports the diagnosis of large cell transformation Mycosis fungoides (MF).
Transformation MF is defined by: -
1. Presence of 25% blastic cells (large cells, 4x reactive lymphocytes).
2. Discrete tumour cell nodule. CD30 positive cells are only seen in ~ 30-50% of cases and is not required in making the diagnosis.
4) MF is defined as epidermotropic PCTCL of small to medium-sized T lymphocytes with cerebriform nuclei. The term should only be used for classical cases (i.e evolution of patches, plaques, and tumours + variants with a similar clinical course).
5) MF is the most common subtype of CTCL, accounting for approximately half of all cutaneous lymphomas. Patients with MF most often experience a protracted clinical course in which disease patches, plaques, and tumors develop over several years or even decades.
6) Some patients, however, undergo a process of large-cell transformation (LCT) which may be characterized by a more aggressive disease course and shortened survival. Early recognition of the clinical clues associated with LCT allows the dermatologist to diagnose this entity earlier and offer patients more aggressive treatment regimens.
7) The prognosis of LCT is reportedly worse than classic MF, and the median survival from diagnosis of LCT has been cited as 37 months for patients with LCT compared with 163 months for those with more classic MF without LCT.
Other studies have reported median survivals as low as 1 month.
REFERENCES:
• Mc Kee’s Pathology of The Skin
• E. Olsen et al. Revisions to the staging and classification of mycosis fungoides and Sézary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood (2007)
• B. Vergier et al. Transformation of mycosis fungoides: clinicopathological and prognostic features of 45 cases. French Study Group of Cutaneous Lymphomas. Blood (2000)
• WHO Classification of Skin Tumours. WHO Classification of Tumours, 4th Edition, Volume 11. Edited by Elder DE, Massi D, Scolyer RA, Willemze R
- Published on
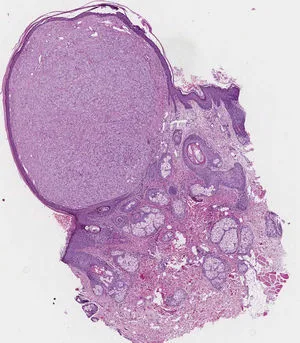
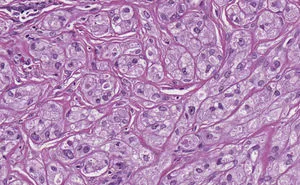
These rare tumors are most commonly reported in the skin, oral cavity, digestive tract, and subcutaneous tissue. However, they can occur anywhere in the body, including breast, bladder, nervous system, respiratory and genitourinary tracts. All age groups and genders can be affected, but it is classically found in women in their 4th to 6th decades of life.Granular cell tumors typically present as solitary, painless nodules less than 3-4 cm large and may be found incidentally.
The vast majority behave indolently. Based on histologic criteria or the presence of metastasis, however, 1% to 2% of these lesions can be malignant, with poor prognosis and few curative options beyond surgical excision.
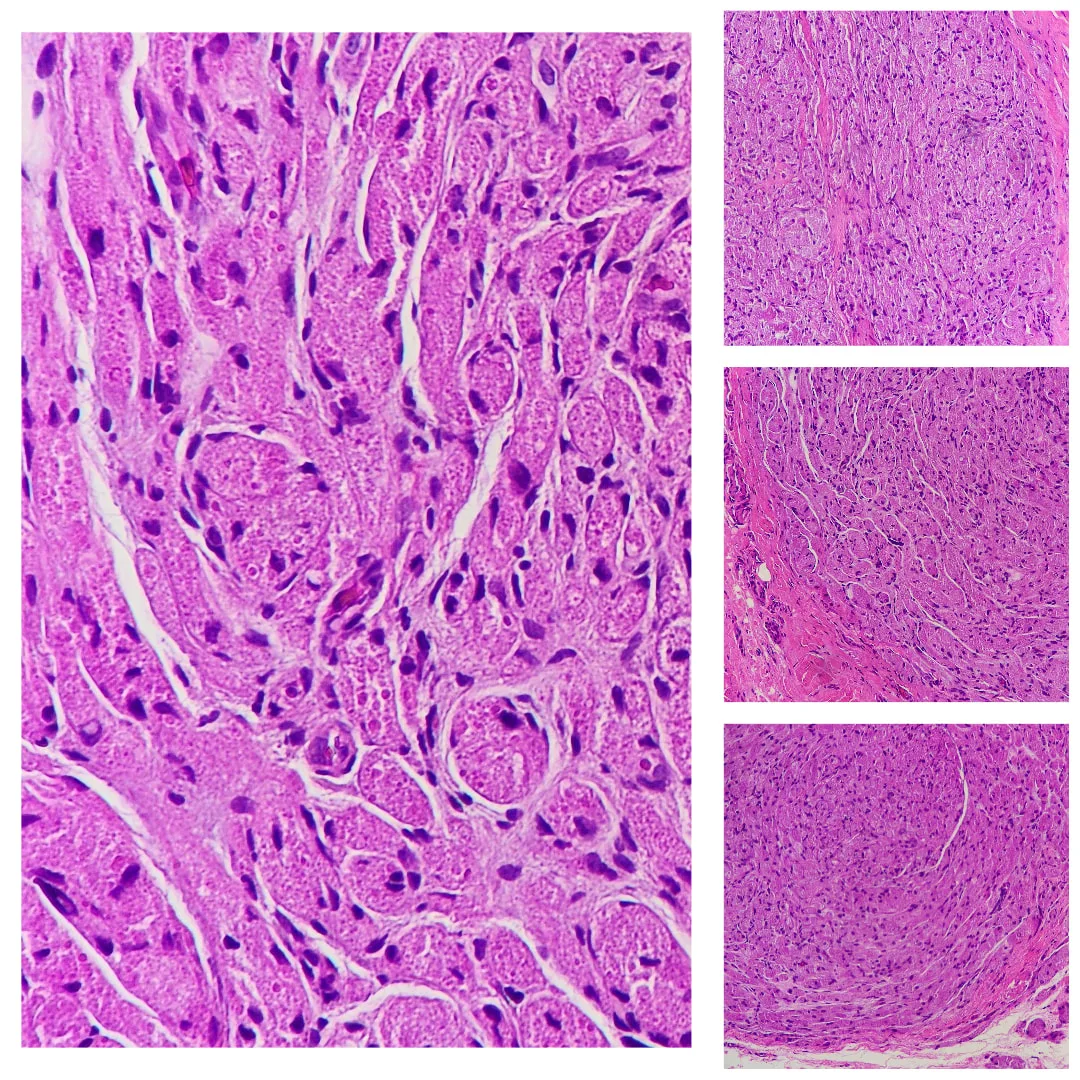
17 years old girl with no known medical illness. C/o swelling over left middle finger for past 1 year. Gradually increasing in size. Pain when pressured eg. picking up object. No limited range of movement. Clinical dx: Left middle finger giant cell tumour (volar)
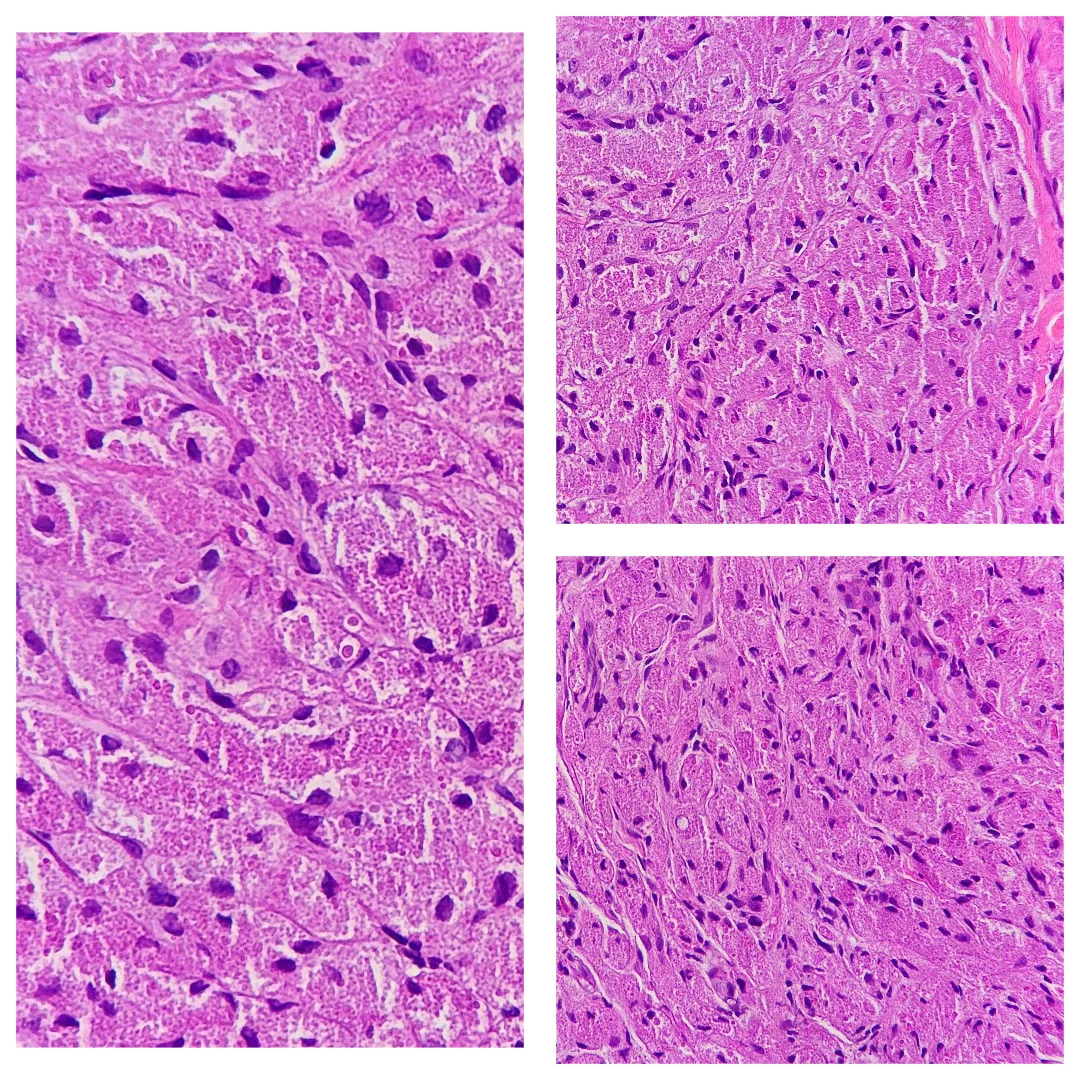
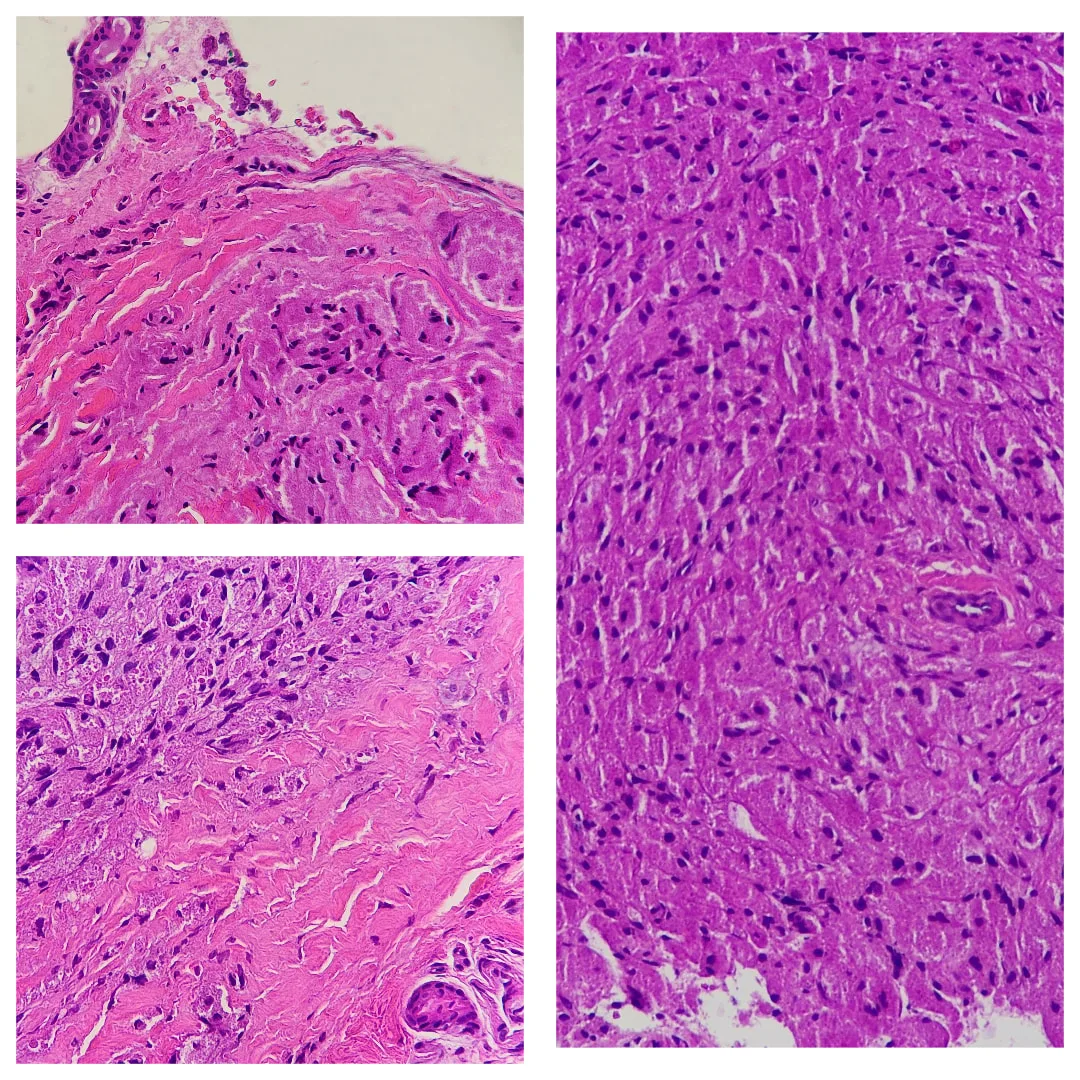
Sometimes, the overlying epidermis may become markedly hyperplastic and mimic a squamous cell carcinoma. This is thought to be a reactive phenomenon.
Malignant forms of granular cell tumour are extremely rare but reported. Frank anaplasia, increased mitotic activity and tumour necrosis are worrisome features.
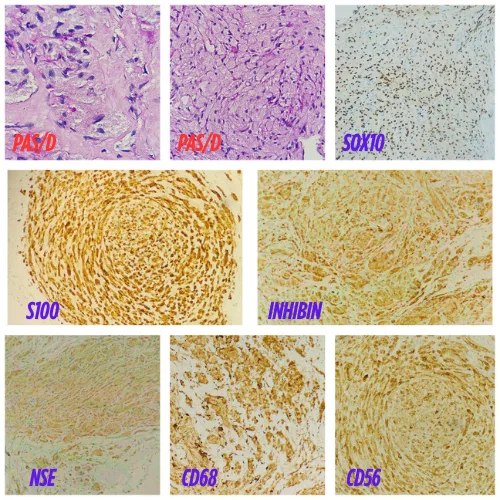
S-100 protein is positive. PAS highlights granules after diastase digestion. Other positive stains may include SOX10 , inhibin , neuron specific enolase, CD68, and CD56.
Differential diagnosis of granular cell tumour pathology :
Rhabdomyoma — These may be similar to granular cell tumour. Rhabdomyomas are positive with desmin and myoglobin.
S-100 immunohistochemical positivity in rhabdomyoma: An underestimated potential diagnostic pitfall in routine practice
Gingival granular cell tumour of newborn ( Congenital epulis of newborn)— These are morphologically similar to granular cell tumour but arise in a distinct clinical setting. S100 is negative.
Other tumours with granular cells – Granular cell change has been described in many other tumours (including dermatofibroma, fibrous papule, AFX and primitive polypoid granular cell tumour - See below). S100 positivity is generally a useful diagnostic aid.
- Published on
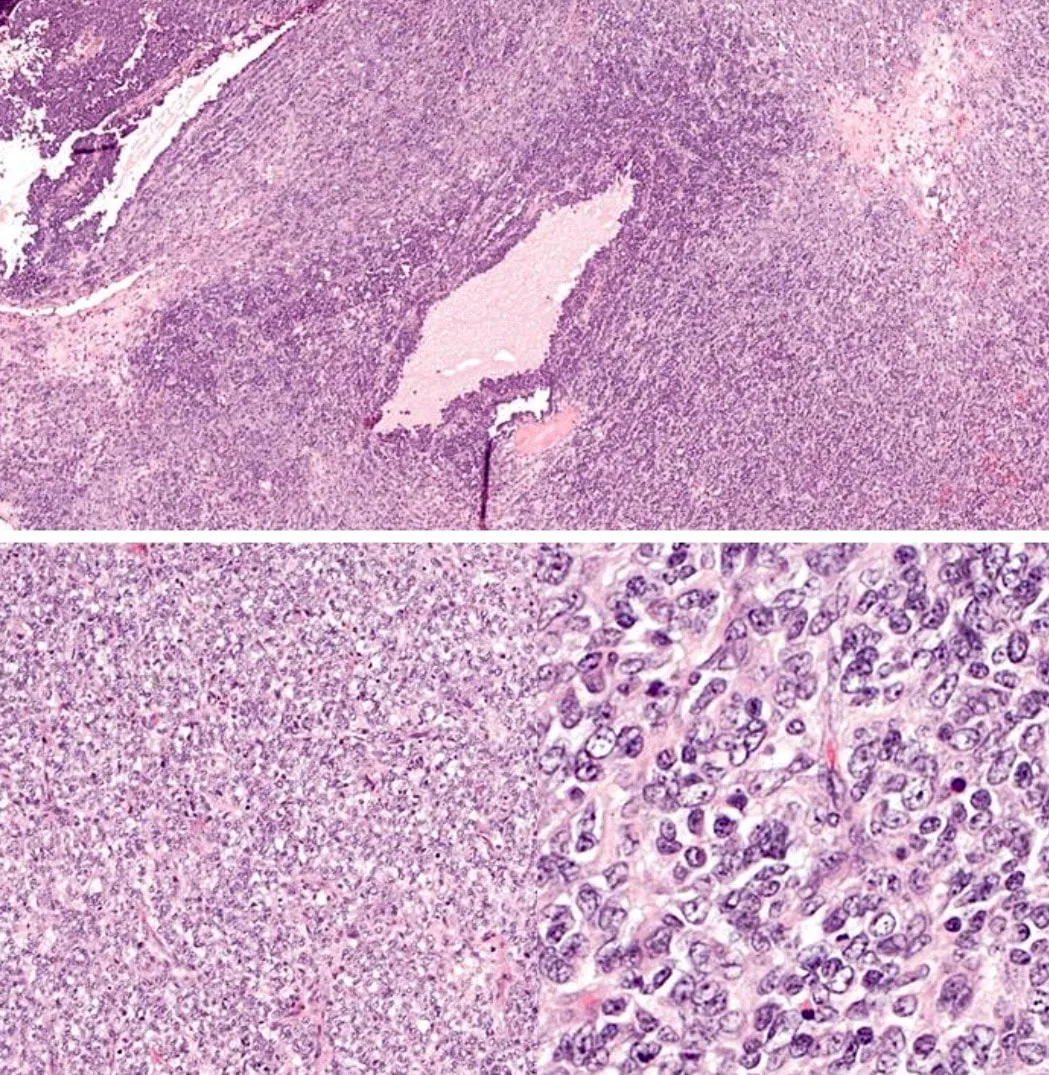
16 y.o, female, abdominal mass, left ovary, high serum calcium. One representative section.
1. The left ovarian mass is composed of diffuse growth of small cells showing irregular round to oval nuclei with small nucleoli. The cytoplasm is scanty. Mitoses are scattered. At focal areas, cystic spaces containing light eosinophilic secretion is observed.
These small cells are focally immunoreactive towards CKMNF116, CD10, calretinin, EMA, and synaptophysin.
They are diffusely positive for WT1.
They are negative for chromogranin and inhibin.
2. Morphologically, the ovarian mass is composed of undifferentiated small cells with a high mitotic count. Small cell carcinoma of hypercalcemic type of the ovary (SCCHT) and granulosa cell tumor of the juvenile type (JGCT) are the main differential diagnoses in this young female patient.
3. In JGCT, follicle-like spaces containing eosinophilic or basophilic secretions are more numerous. JGCT may have fibrous septa and fibrothecomatous component. In contrast, SCCHT has focal follicle-like spaces with scanty stroma. The most useful immunohistochemical marker to differentiate between these two is inhibin whereby it is positive in JGCT but negative in SCCHT.
4. Clinically, SCCHT is usually associated with hypercalcemia whereas JGCT with estrogenic manifestations.
5. JGCT mostly presents at stage I with excellent prognosis whereas SCCHT is a highly aggressive tumor with a poor prognosis (almost all patients with a stage higher than stage Ia died of disease)
Reference
1. Soslow, R. A., & Tornos, C. (Eds.). (2011). Diagnostic pathology of ovarian tumors. Springer Science &
Business Media.
2. Kurman, R. J., Carcangiu, M. L., Herrington, C. S., & Young, R. H. (2014). WHO classification of tumours of
female reproductive organs. Lyon: International Agency for Research on Cancer.
- Published on

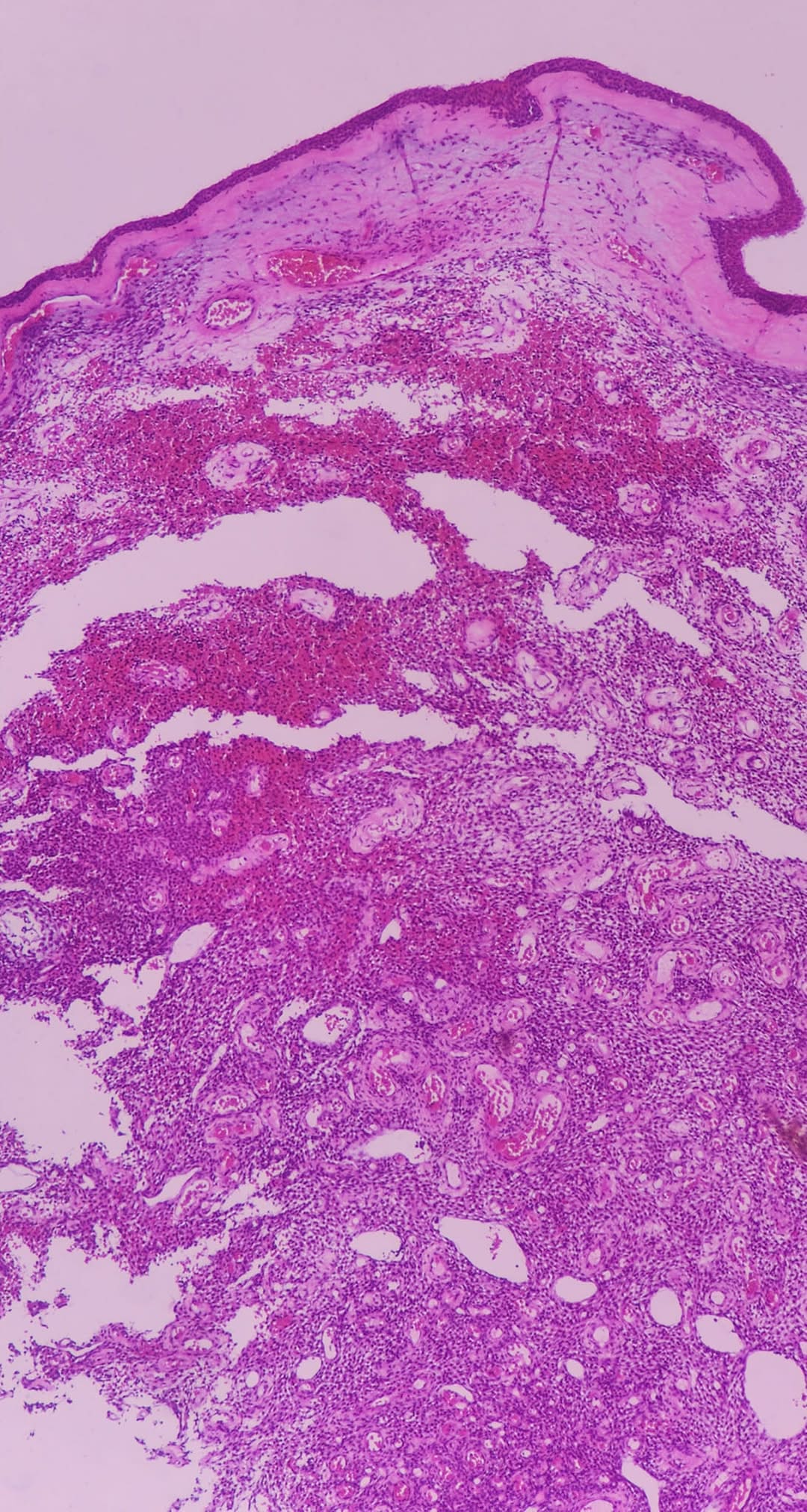
54 yo lady presented with right neck swelling. O/e Bilateral postnasal space mass extending up to the anterior ethmoidal and sphenoidal sinuses. Biopsies of both right and left postnasal spaces show nasopharyngeal carcinoma. In addition, biopsy of the right postnasal space also shows a coexisting polypoid lesion (Collision tumors).
The understanding and classification of sinonasal glomangiopericytoma have evolved over time. Initially reported in 1942 by Stout and Murray, it was first categorized under the broader term of hemangiopericytoma . At the time, it was hypothesized that this lesion resided within the spectrum of tumors connecting glomus tumors and capillary hemangiomas . Over the years, the term "sinonasal-type hemangiopericytoma" gained traction when referring to these specific lesions arising in the nasal cavity or paranasal sinuses . A significant milestone in the classification of this tumor occurred in 2005 when the World Health Organization (WHO) formally recognized it as a distinct entity and designated it as glomangiopericytoma (GPC) . This classification acknowledged its unique perivascular myoid phenotype and its resemblance to glomus tumors . This distinction was based on differences in location, biological behavior, and histological characteristics when compared to conventional soft tissue hemangiopericytomas . The WHO's classification also listed 'glomangiopericytoma' and 'myopericytoma' as synonyms . Before 2021, this entity was coded under the classification of hemangiopericytoma with the code 9150/3 . This historical perspective highlights the increasing recognition of GPC as a unique tumor type with specific features and behavior.
Epidemiological studies reveal that sinonasal glomangiopericytoma is indeed a rare tumor, with an incidence of less than 0.5% of all sinonasal neoplasms . Some studies indicate it accounts for approximately 0.5% of all nose and sinus neoplasms and less than 1% of all sinonasal tumors . Interestingly, GPC is estimated to represent about 5% of all hemangiopericytomas . The age distribution of diagnosed patients typically falls within the 6th or 7th decade of life , with a peak incidence observed in the seventh decade . However, the tumor can affect a broad age range, from 5 to 90 years, with the mean age being in the seventh decade . Generally, it tends to affect individuals between 40 and 60 years of age . Regarding gender, there is often a slight female predominance reported , with a female to male ratio of approximately 1.2 to 1 . However, some studies have shown a predominantly male incidence , while others report no significant difference between the sexes . In terms of location, GPC is generally localized to the nasal cavity , with paranasal involvement and skull base extension being uncommon . When the paranasal sinuses are involved, the ethmoid and sphenoid sinuses are most frequently affected . The maxillary and ethmoid sinuses can also be involved in conjunction with the nasal cavity , and lone involvement of a paranasal sinus has been documented . Bilateral tumors are rare, occurring in approximately 5% of cases . While the nasal cavity is the most common site, isolated involvement of the turbinate and septum can occur . Occurrence in the nasopharynx is rare , and even less frequently, it can be found in other locations like the spinal cord or the pterygomandibular space .
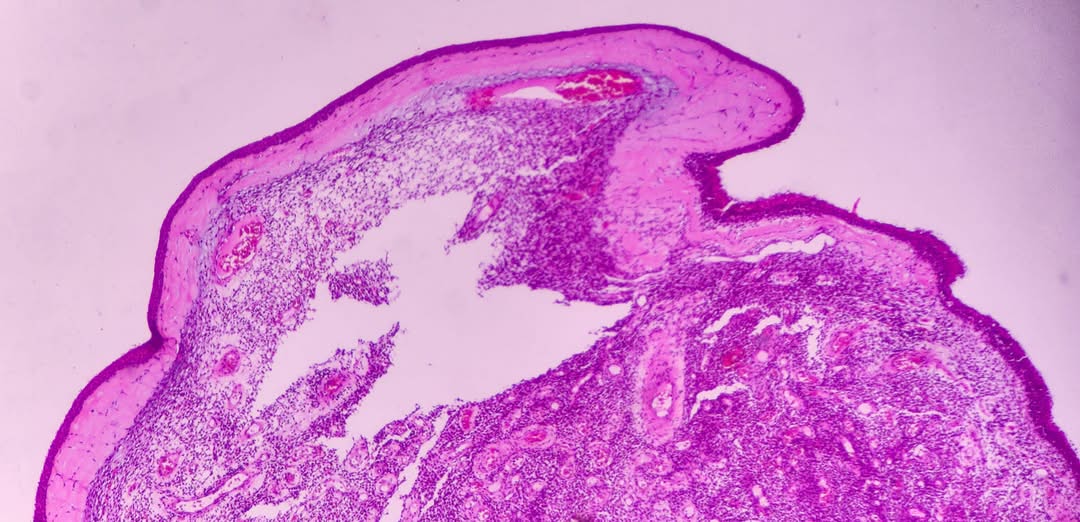
The clinical presentation of sinonasal glomangiopericytoma often involves non-specific symptoms related to a mass effect within the nasal cavity or paranasal sinuses. The most common symptoms reported by patients include nasal obstruction and epistaxis (nosebleeds) . Other frequently reported symptoms include headache and facial pain or pressure , as well as sinusitis . Less common symptoms can include anosmia (loss of smell) , difficulty breathing , visual disturbance , serous otitis media , proptosis (eye bulging) , infraorbital anesthesia , hyposmia (reduced sense of smell) , facial numbness , disturbance in smell or taste , nasal pain , local swelling , and in rare cases of cavernous sinus extension, mild left-sided ptosis . Macroscopically, sinonasal glomangiopericytoma may resemble common inflammatory polyps and often presents as a polypoid mass . These masses are frequently described as reddish and polypoidal , often being friable and prone to bleeding upon manipulation . Some reports describe them as solid, firm, red or fleshy, soft, and hemorrhagic polypoid edematous masses with a mean size of 3.1 cm (ranging from 1 to 8 cm) . They can also appear as beefy red to grayish pink with hemorrhage and have a soft, edematous, and fleshy cut surface . In some instances, the tumor may present as a purplish mass with a gelatinous aspect and friability on biopsy . Due to the fragmentation that often occurs during endoscopic removal, the gross appearance is generally not very helpful . However, if intact, the tumor may exhibit solid, soft, fleshy, or friable cut surfaces with hemorrhagic and/or edematous areas, typically ranging from 1 to 8 cm with an average of 3.1 cm . They can also appear as beefy red or fleshy pink, polypoid, hemorrhagic masses that bleed easily when palpated, with a mean size of approximately 3 cm .
Computed tomography (CT) is a valuable tool for assessing the extent of the tumor and identifying any potential involvement of the bone . On CT scans, GPCs typically appear as well-defined masses that exhibit uniform enhancement after the administration of contrast . Magnetic resonance imaging (MRI) offers superior soft tissue contrast, making it particularly useful for delineating the tumor's relationship with adjacent structures . MRI often reveals a mass with well-defined borders that enhances with contrast and may show bone erosion without dural enhancement . While the appearance on CT and MRI can be non-specific, imaging plays a crucial role in differential diagnosis, assessing the tumor's extent and size, and suggesting non-aggressive characteristics prior to surgical intervention . On MRI, the tumor may be isointense to brain parenchyma on T1 and T2 sequences, without restricted diffusion, and show homogenous contrast enhancement . CT without contrast may demonstrate a mass isodense to soft tissue, lacking calcification, but showing arterial enhancement . Coronal CT in bone windows can highlight bone erosion, while coronal CTA in soft tissue windows demonstrates arterial enhancement. Coronal T2 MRI may show isointensity relative to brain parenchyma, and coronal T1 post-contrast MRI typically displays homogenous enhancement . CT often reveals a soft-tissue mass with strong enhancement after contrast, potentially mimicking an inflammatory polyp . On T1-weighted MRI, the mass appears solid isointense with strong contrast enhancement, whereas on T2-weighted images, the signal intensity can vary from iso- to hypo-intense, which can help differentiate it from high-intensity inflammatory fluid . The typical signal characteristics on MRI include T1 isointense to muscle, T2 heterogeneous high signal intensity, and vivid enhancement on T1 with gadolinium contrast . GPCs often appear hyperintense on T2-weighted images and may exhibit vascular signal voids . Diffusion-weighted imaging (DWI) may show a high mean apparent diffusion coefficient (ADC) value , and dynamic contrast-enhanced MRI can reveal a wash-in and washout pattern . Both CT and MRI may show a polypoid mass that can be lobulated and sometimes associated with bone erosion or sclerosis .
Endoscopic examination is essential for visualizing the sinonasal mass. Sinonasal hemangiopericytoma often presents as a polypoid mass on endoscopy , appearing as a soft, fleshy, polypoidal, beefy red to greyish mass . Macroscopically, GPC lesions can closely resemble inflammatory polyps during endoscopic evaluation . Clinical symptoms often correlate with the presence of a polypoid mass identified in the nasal cavity during endoscopy , which may appear as a red to grayish polypoid soft mass or a bright red polypoid mass attached to the septum . Endoscopy is also used in the preoperative workup to assess the extent, size, and characteristics of the tumor . However, the definitive diagnosis of sinonasal glomangiopericytoma is achieved through tissue sampling, either after complete surgical resection or via biopsy .
Biopsy specimens often reveal soft tissue with perivascular myoid differentiation, along with positive staining for specific immunohistochemical markers . Grossly, the tumor may present as a purplish mass with a gelatinous appearance and friability on biopsy . It can also appear as a polypoid mass, averaging 3 cm in size, with a beefy red to grayish pink color and hemorrhage, often having a soft, edematous, and fleshy cut surface . Frozen sections examined during surgery may show specific histological features indicative of GPC .
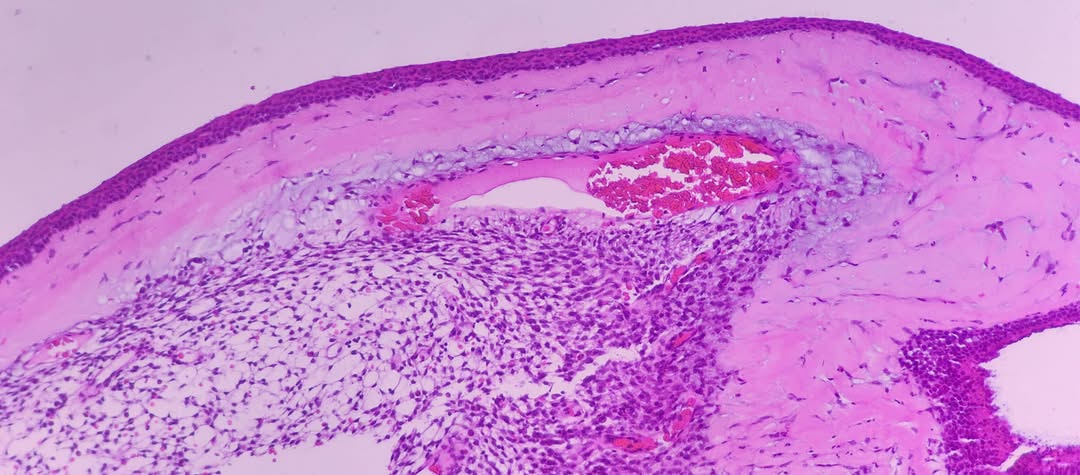
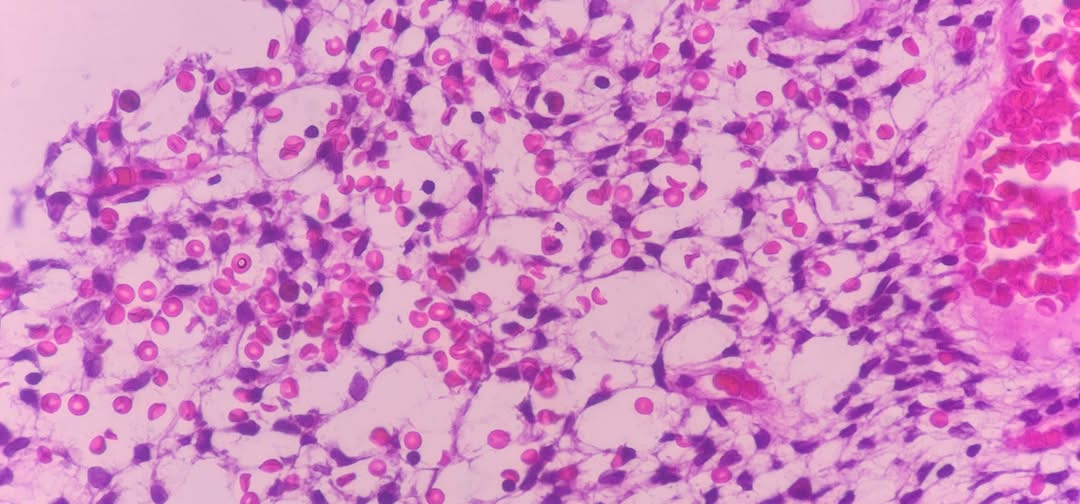
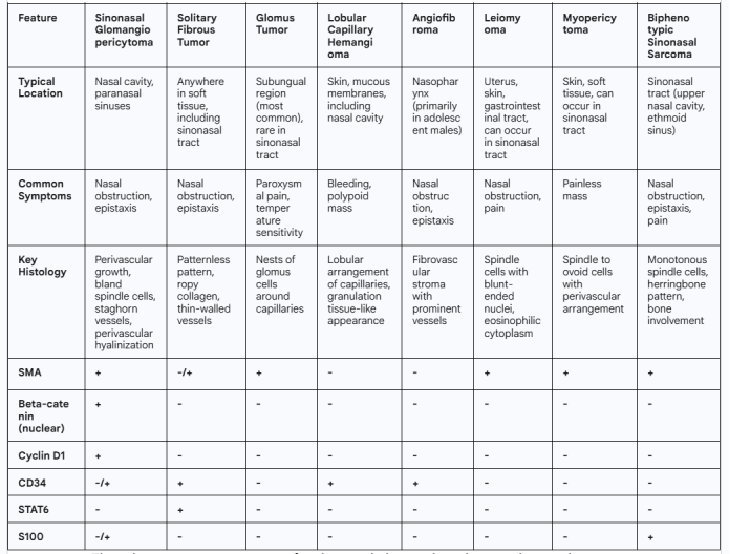
Microscopically, sinonasal glomangiopericytoma is characterized by a proliferation of spindle-shaped cells arranged around blood vessels . These closely packed spindle cells are uniform with bland nuclei and are surrounded by a distinctive vascular network featuring thin-walled, branching vessels often described as having a "staghorn" appearance . The tumor typically exhibits a diffuse, subepithelial proliferation of bland, uniform, closely packed spindled cells growing in various patterns . A distinctive vascular network composed of variably sized vascular channels, with smaller channels showing perivascular hyalinization, is often present . Histologically, it is an unencapsulated tumor located beneath the epithelium, separated by a Grenz zone, and contains many ectatic staghorn-type vessels. The tumor cells are bland oval with spindled nuclei and eosinophilic cytoplasm .
Key features include a subepithelial Grenz zone, hemorrhagic stroma, perivascular proliferation and hyalinization, and staghorn vessels . The growth pattern is often diffuse with fascicular, solid, or focally whorled arrangements of spindled or round/oval tumor cells surrounding prominent, small, thin-walled submucosal blood vessels. Minimal cellular atypia, absence of necrosis, and rare mitotic activity are typical .
Unlike glomus tumors, the eosinophilic cytoplasm in GPC results in a syncytial appearance due to the lack of distinct cell borders. The nuclei are oval with smooth contours, even, pale-staining chromatin, and one or more small nucleoli . GPC is a cellular spindle cell neoplasm characterized by hemangiopericytoma-like vessels and frequent perivascular hyalinization of the capillary-sized vessels . It may also show diffuse and fascicular growth, as well as storiform or whorled patterns . Most tumors contain inflammatory cells and extravasated red blood cells. While mild cytologic atypia and occasional mitotic figures may be observed, necrosis is typically absent. In contrast to the more common low-grade GPC, malignant forms can exhibit high mitotic activity, necrosis, nuclear pleomorphism, and bone invasion .
Immunohistochemical analysis is crucial for confirming the diagnosis. GPCs typically show positive staining for α-smooth muscle actin (SMA), indicating myoid differentiation , as well as for vimentin and beta-catenin, with nuclear staining being a characteristic feature . Cyclin D1 is also typically positive , as is CD99 . Factor XIIIa is often positive , while staining for desmin, cytokeratin, and S100 protein is usually negative .
However, focal and weak positivity for CD34 and S100 protein can occur in a small percentage of tumors . In some cases, positive reactivity to CD34 has been observed . In one reported case, the tumor was negative for desmin, CD31, ERG, CD34, and AE1/AE3 .
Muscle-specific actin is also typically positive , and STAT6 is usually negative . Laminin can be positive in some instances , and markers like Bcl-2, CD99, CD117, and cytokeratins are typically negative . Recent research has also indicated that TLE1 can be positive in all cases in some studies .
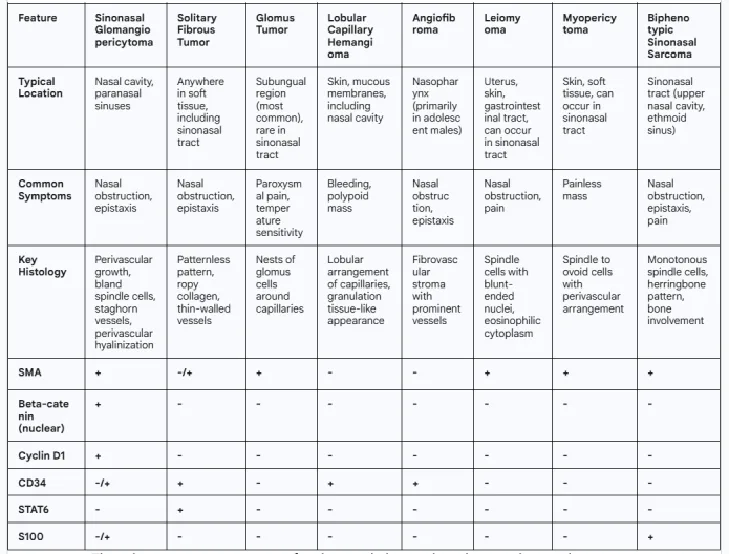
The differential diagnosis of sinonasal glomangiopericytoma is broad and includes several other spindle cell and vascular tumors that can occur in the sinonasal tract. Key entities to consider include solitary fibrous tumor (SFT) , lobular capillary hemangioma (pyogenic granuloma) , leiomyoma , angiofibroma (juvenile nasopharyngeal angiofibroma) , glomus tumor , myopericytoma , synovial sarcoma , spindle cell hemangioma , kaposiform hemangioendothelioma , Kaposi sarcoma , desmoid type fibromatosis , cellular hemangioma , epithelioid tumors , schwannoma , vascular leiomyoma , angioleiomyoma , hemangioendothelioma , histiocytoma , chondrosarcoma , endocrine tumors , Ewing or Ewing-like sarcoma , sinonasal smooth muscle tumors (leiomyoma and leiomyosarcoma) , peripheral nerve sheath tumors (benign and malignant) , and biphenotypic sinonasal sarcoma (BSNS) .
GPC differs from conventional soft tissue hemangiopericytoma in its location, biological behavior, and histological features, tending to be more indolent . The presence of strong nuclear β-catenin expression in GPC is a key feature often associated with CTNNB1 gene mutations . Unlike other soft tissue hemangiopericytomas, GPC typically shows positive staining for smooth muscle actin and cyclin D1 .
Solitary fibrous tumor is characterized by abundant collagen, positivity for bcl-2 and CD34, and negativity for actin, which helps distinguish it from GPC .
Glomus tumor, another pericytic tumor, is extremely rare in the sinonasal region and is composed of compact epithelioid cells, positive for SMA but negative for beta-catenin nuclear staining .
Lobular capillary hemangioma exhibits a lobular pattern, spindled fibroblasts, prominent small capillaries, and is positive for CD34 and CD31 but negative for beta-catenin nuclear staining .
Solitary fibrous tumor shows a patternless pattern with ropy keloidal collagen and thin-walled vascular spaces, staining positive for CD34 and STAT6 but negative for beta-catenin nuclear staining .
Ewing or Ewing-like sarcoma is characterized by tumor cells with clear cytoplasm and positivity for CD99, along with negative staining for beta-catenin nuclear staining and positivity for EWSR1 rearrangement .
In cases with intracranial extension or involvement of the pterygopalatine fossa, endoscopic surgical excision is still considered a viable option and not necessarily a contraindication . However, in advanced cases, open surgical approaches such as medial maxillectomy may be required . For tumors with orbital extension, a combined surgical approach involving both endoscopic and trans-sinusal frontal approaches may be necessary to achieve complete removal and address any bony defects .
Given the vascular nature of glomangiopericytomas, particularly large or highly vascular tumors, preoperative selective embolization can be a beneficial adjunct to surgery . This procedure aims to reduce intraoperative bleeding and facilitate more complete tumor resection . Preoperative embolization with microparticles followed by complete endoscopic resection has been reported in several cases . Angiography can be used preoperatively to map the tumor's vascular supply, aiding in surgical planning and embolization to minimize bleeding risks . Transarterial embolization is specifically indicated in some instances to prevent massive surgical hemorrhage . While preoperative embolization of afferent vessels can help reduce blood supply and facilitate surgical resection , there is currently no universal consensus regarding its routine use .
The role of radiation therapy and chemotherapy in the management of sinonasal glomangiopericytoma is limited. GPC tumors are generally considered relatively resistant to both radiation and chemotherapy . In some instances, these modalities may be used as palliative approaches . These neoplasms tend to be radioresistant, with surgery being the most effective treatment . However, in cases of metastatic disease, a combination of radiotherapy and chemotherapy might be considered as adjunctive or palliative therapy . Limited data suggest that radiotherapy following incomplete surgical resection may lower the rate of recurrence , but the overall role of chemo and radiotherapy remains controversial . Generally, these therapies are less effective and are reserved for recurrent disease or palliative management .
The prognosis for sinonasal glomangiopericytoma after complete surgical resection is generally excellent , with a reported 5-year survival rate greater than 90% in many cases . The overall survival rate is typically long , and 5-year overall and disease-free survival rates of 88.1% and 74.2%, respectively, have been reported . However, local recurrence is a significant concern, with rates ranging from 7% to as high as 40% in some studies . Some reports indicate a recurrence rate of approximately 27% , while others note high recurrence rates and even long-term local recurrence rates up to 50% , often attributed to incomplete resections. Recurrences can occur late, sometimes years after the initial treatment, with up to 40% happening more than 5 years post-surgery . Local recurrences have been reported as late as 12 years after the initial excision . Factors associated with recurrence include a long duration of symptoms, bone invasion, and profound nuclear pleomorphism . In contrast to the relatively high local recurrence rate, metastasis is extremely rare , with rates estimated at around 5–10% and typically preceded by multiple local recurrences . Aggressive behavior of the tumor is generally uncommon . Due to the risk of late recurrences, long-term surveillance is crucial. Post-operative care should include regular nasal endoscopy and potentially radiological examinations .
p/s: Nasopharyngeal carcinoma (NPC) can coexist with other lesions, sometimes referred to as collision tumors, where multiple distinct tumors occur in the same organ. These can include lymphoma, extramedullary plasmacytoma, or other cancers. A collision tumor refers to the simultaneous occurrence of two or more different types of tumors in the same organ or tissue. Recognizing the presence of multiple tumors is crucial for accurate diagnosis and appropriate treatment planning. The rarity of these coexisting lesions can lead to diagnostic challenges, potentially resulting in misdiagnosis and improper management. The presence of multiple tumors can affect the prognosis and treatment outcomes. Distinguishing between different tumor types in the same tissue can be challenging for pathologists. Imaging techniques like MRI can help identify different components of collision tumors and can help determine the extent of the lesion.
- Published on
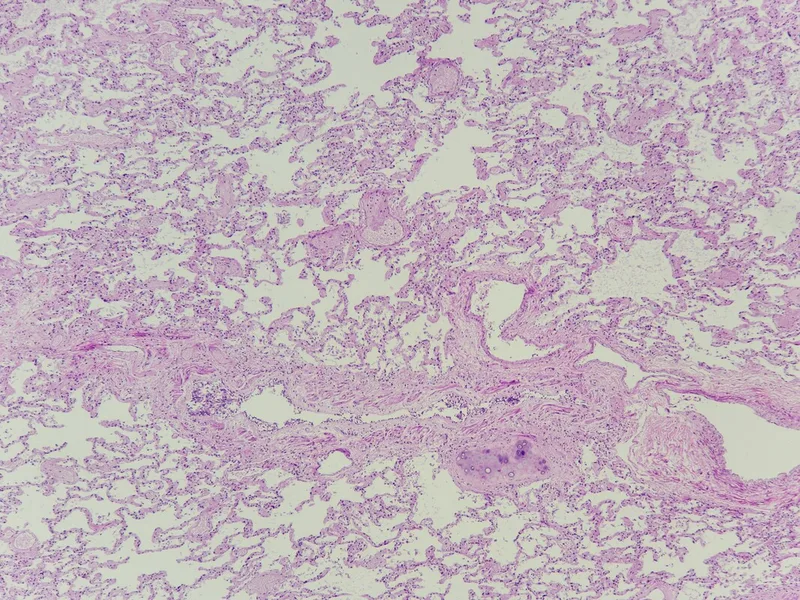
Case 2 - 43 years old lady with severe dengue. Incidental finding during postmortem: Right upper lobe lung nodule.
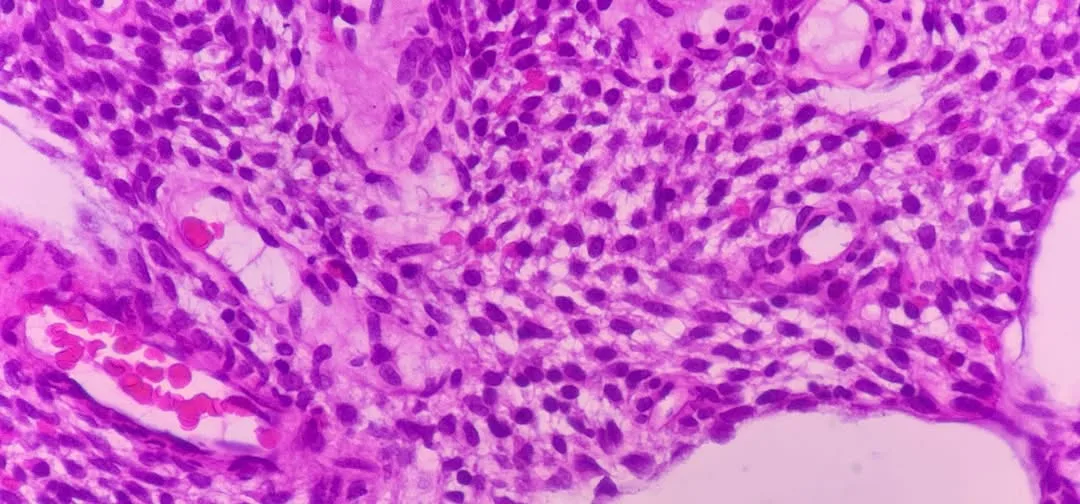
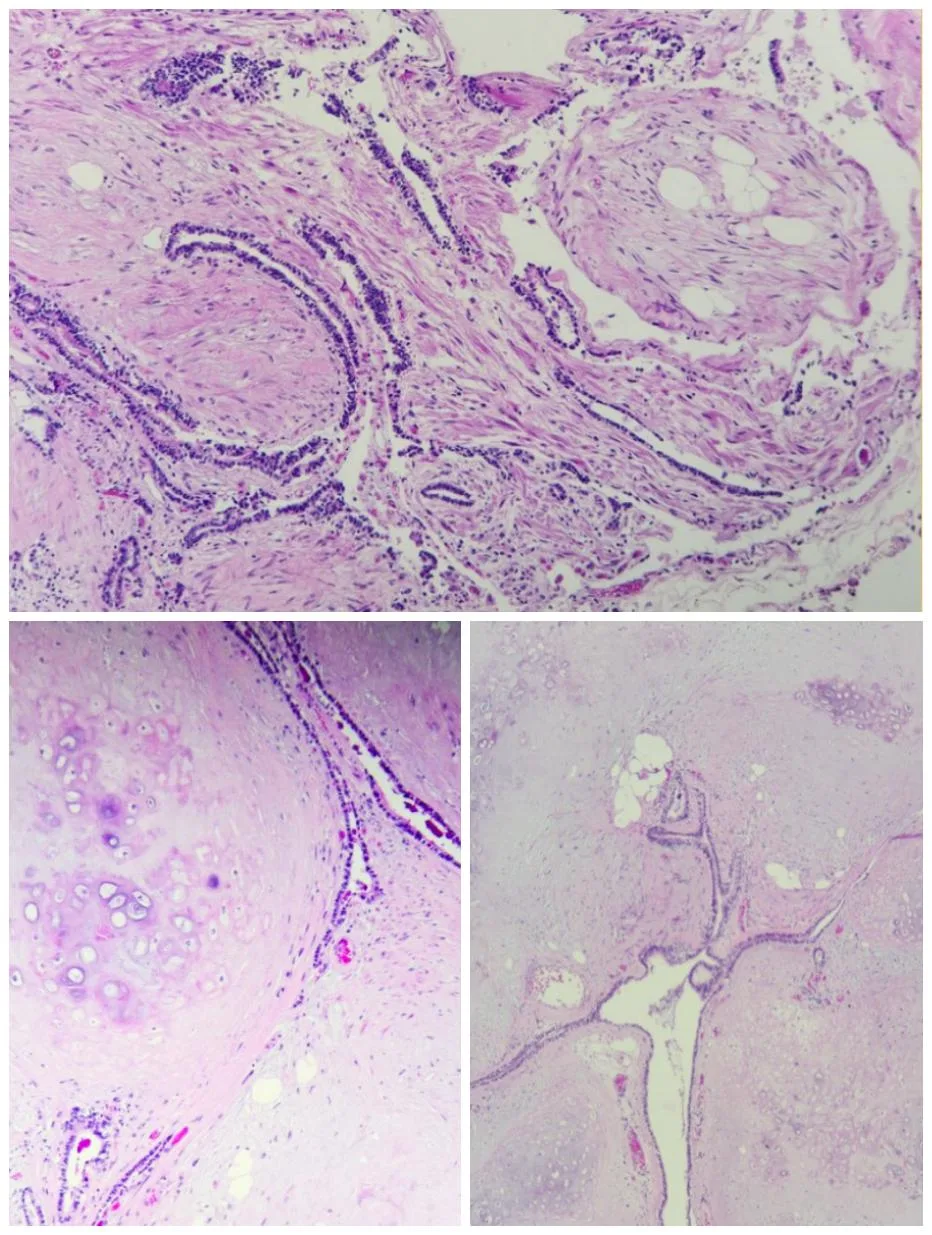
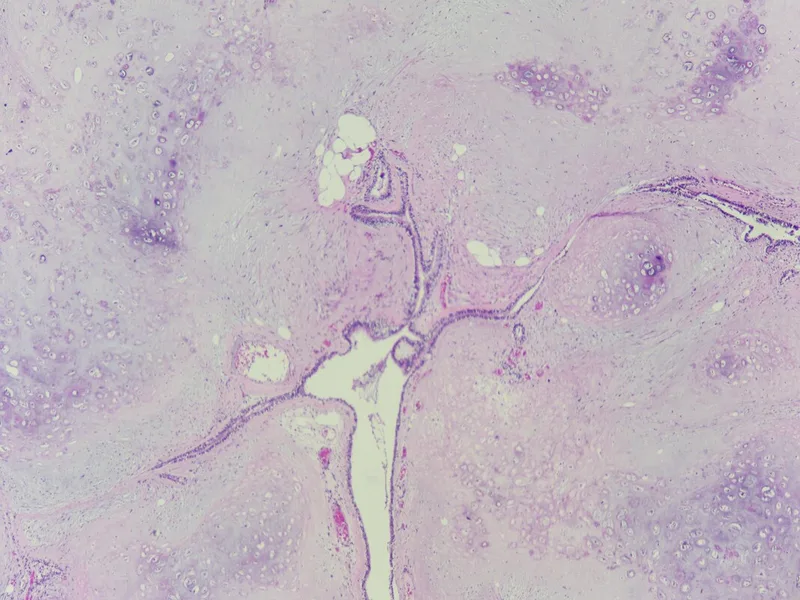
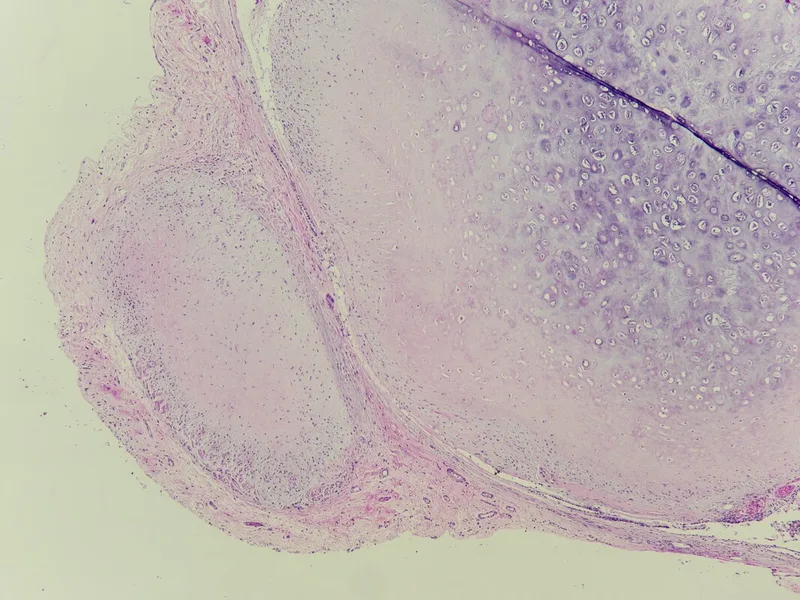
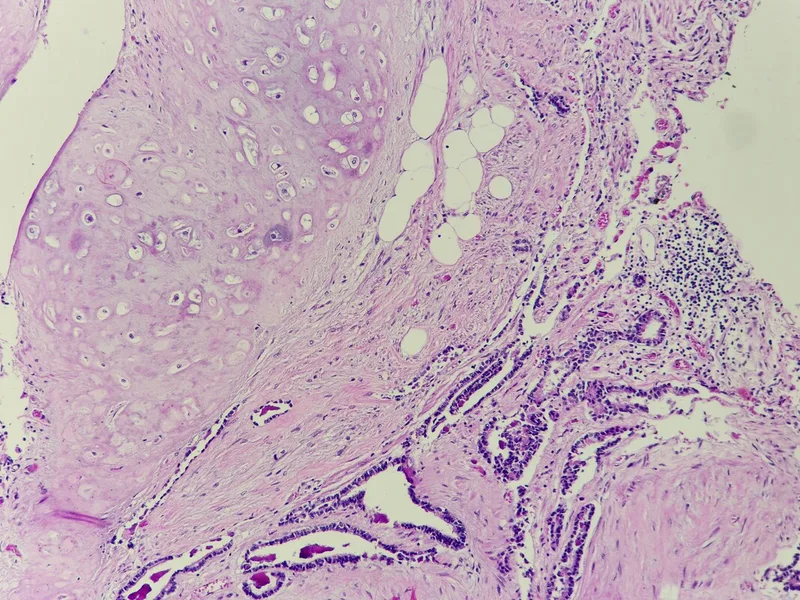
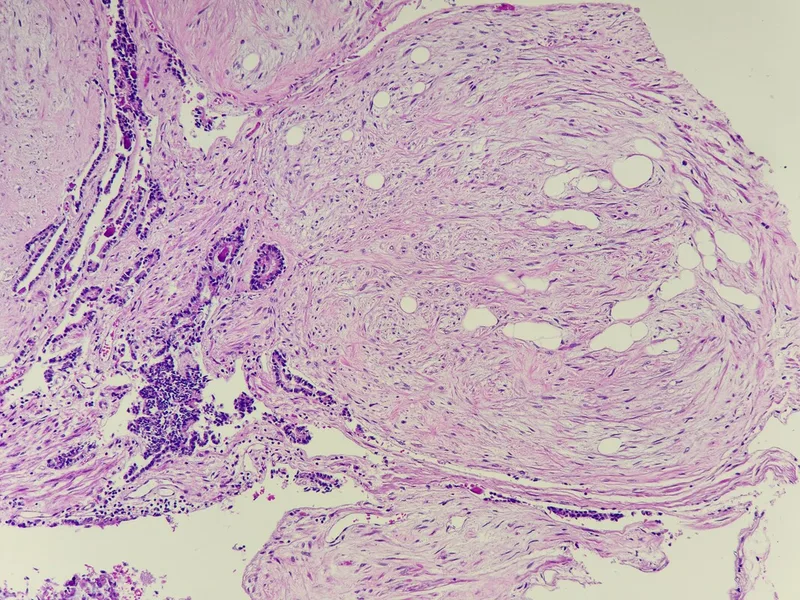
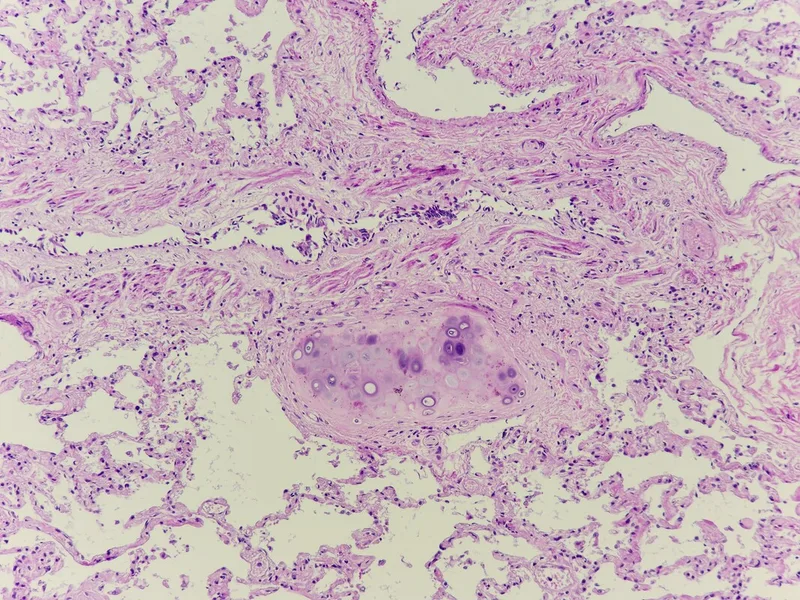
Histopathology of pulmonary hamartoma:
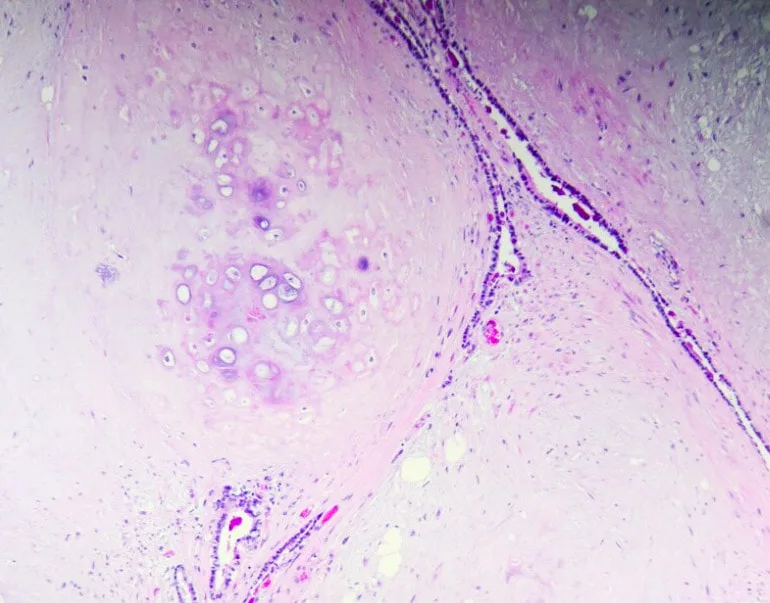
* Gross appearance: Pulmonary hamartomas are typically well-circumscribed, solitary nodules that can range in size from a few millimeters to several centimeters (Most are less than 40 mm) . They often have a firm, rubbery texture and may have a gritty or calcified feel due to the presence of cartilage.
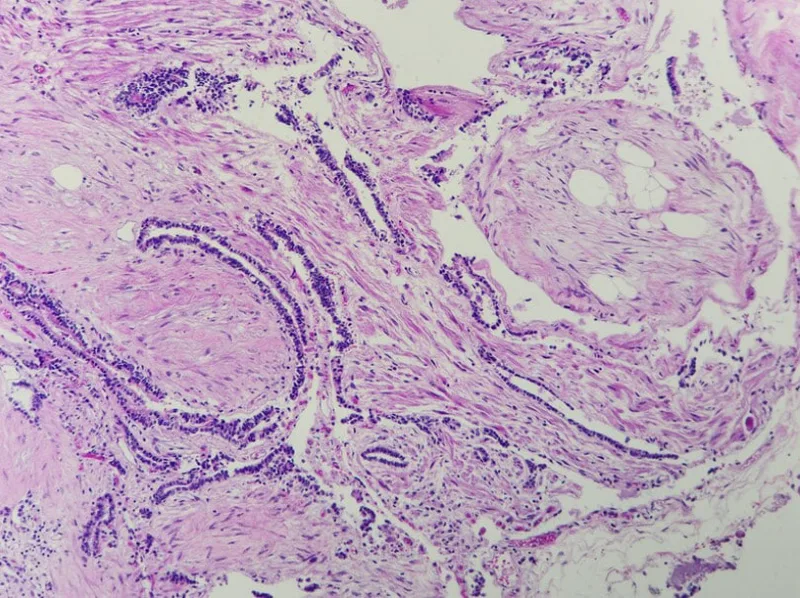
* Microscopic appearance: Histologically, pulmonary hamartomas are characterized by a haphazard arrangement of mature mesenchymal elements, such as cartilage, fat, bland myxoid spindle cells, smooth muscle, fibrous connective tissue and bone, interspersed with islands of respiratory epithelium. The cartilage is often hyaline or fibrocartilaginous and may show calcification or ossification. The fat cells are mature adipocytes. The smooth muscle cells are arranged in bundles or sheets. The respiratory epithelium is typically normal and may line cysts or alveolar spaces.
Key features for diagnosis:
* Presence of at least two different benign mesenchymal elements (e.g., cartilage and fat, cartilage and smooth muscle, or fat and myxoid spindle cells)
* Entrapment of respiratory epithelium within the mesenchymal elements
Additional notes:
* Pulmonary hamartomas are usually benign and do not require treatment unless they are causing symptoms or are large enough to be mistaken for a malignancy.
* In rare cases, pulmonary hamartomas may be associated with other conditions, such as Carney triad, which is a syndrome that includes pulmonary hamartoma, functioning extra-adrenal paragangliomas, and gastrointestinal stromal tumors.
* Monomorphic soft tissue tumours - Presence of more than one mesenchymal component in pulmonary hamartoma.
* Pulmonary chondromas - Typically arise in patients with Carney triad and lack entrapped epithelium. SDHB immmunohistochemistry may be useful; it shows abnormal loss in Carney-associated chondroma , but not in pulmonary hamartoma.
* Endobronchial lipoma Vs lipomatous hamartoma, whereas epithelial inclusions tend to be inconspicuous- Distinction is generally not critical.
* If only myxoid spindle cell component is sampled - which could lead to consideration of myxoid periheral nerve sheath tumour or even myxoid sarcoma - Unlike those of sarcomas, the spindle cells of hamartoma are generally very bland, without atypia, and they have very low cellularity.
- Published on
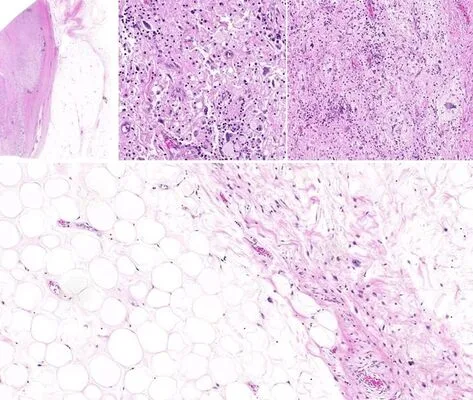
Case 1: A 55 years old man presented with a left paratesticular mass
1. This para-testicular mass is a dedifferentiated liposarcoma (LPS) showing transition of a well differentiated liposarcoma (LPS) to non-lipogenic sarcoma. The dedifferentiated lipomatous component is composed of scattered marked pleomorphic malignant cells set in an edematous inflammatory stroma. Some of the malignant cells are in multinucleated form.
The nature of this malignant tumor is revealed with the presence of the adjacent well differentiated LPS. The well-differentiated LPS is composed of mostly mature adipose showing marked variation in size and shape. Atypical stromal cells displaying enlarged hyperchromatic nuclei are seen within the fibrous septa. Occasional adipocytes with atypical enlarged hyperchromatic nuclei are also seen.
2. Dedifferentiated LPS is usually a non-lipogenic sarcoma of variable histological grades. The diagnosis of dedifferentiated LPS lies in recognition of progression of an atypical lipomatous tumor/ well-differentiated LPS in the primary or in a recurrence.
3. Nonetheless, the well-differentiated component may not be identifiable in some cases.
Diffuse nuclear expression of MDM2 and/or CDK4 immunohistochemistry or demonstration of MDM2 gene amplification by FISH would be helpful to differentiate dedifferentiated LPS from other high-grade sarcomas in the appropriate setting, especially in the case of sarcomas arising in the retroperitoneum and spermatic cord.
4. Dedifferentiated LPS has a high local recurrence (at least 40%) and develops distant metastases in 15-20%. Nevertheless, as compared to the other high-grade sarcomas, dedifferentiated LPS has a less aggressive clinical course.
Reference:
1. WHO Classification of Tumours Editorial Board. Soft tissue and bone tumours [Internet]. Lyon (France): International Agency for Research on Cancer; 2020