Case 9 - A 46 y.o. LADY
was diagnosed with adenocarcinoma in situ on pap smear and she underwent cervical cone biopsy. One representative section.
🎯𝘛𝘈𝘙𝘎𝘌𝘛𝘌𝘋 𝘋𝘐𝘈𝘎𝘕𝘖𝘚𝘐𝘚 🎯
- Published on
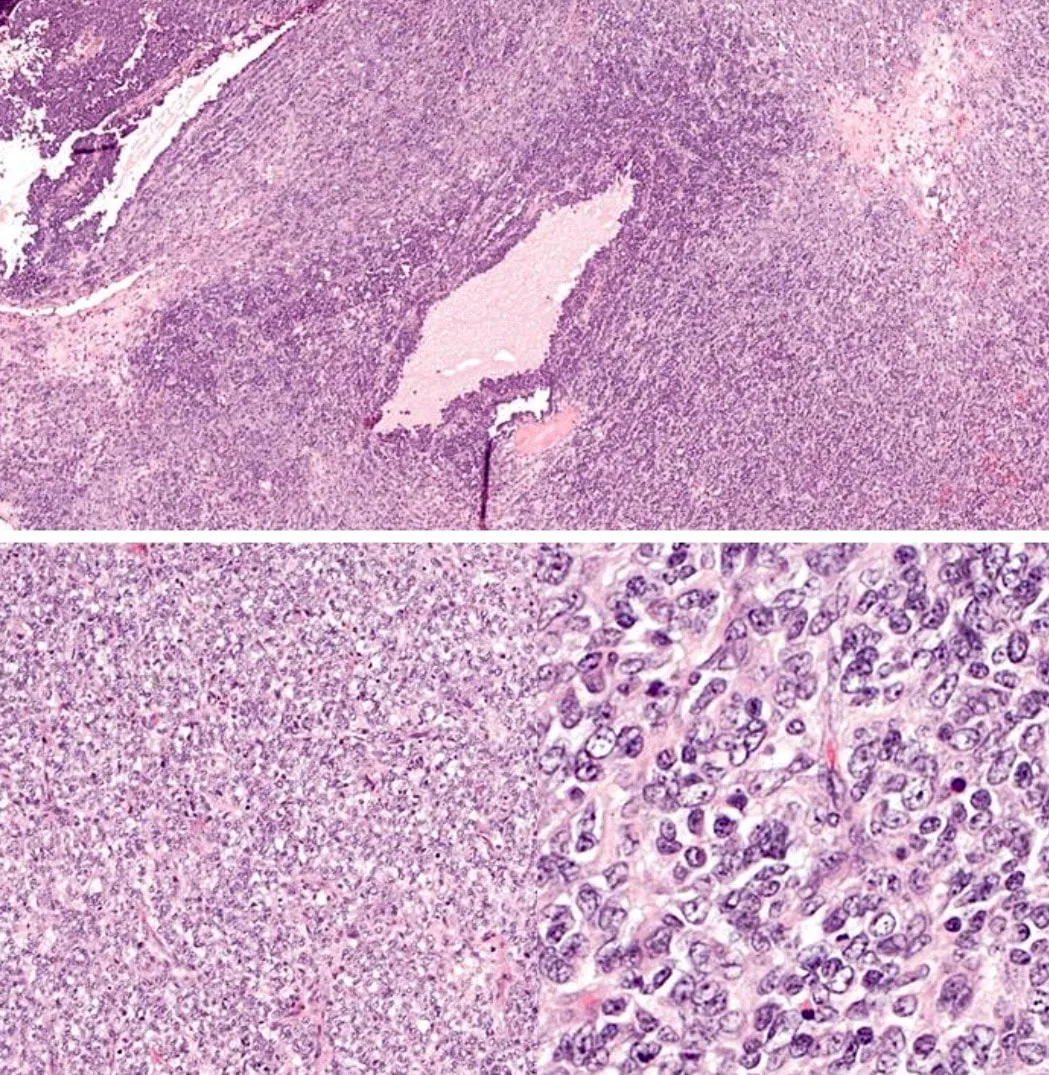
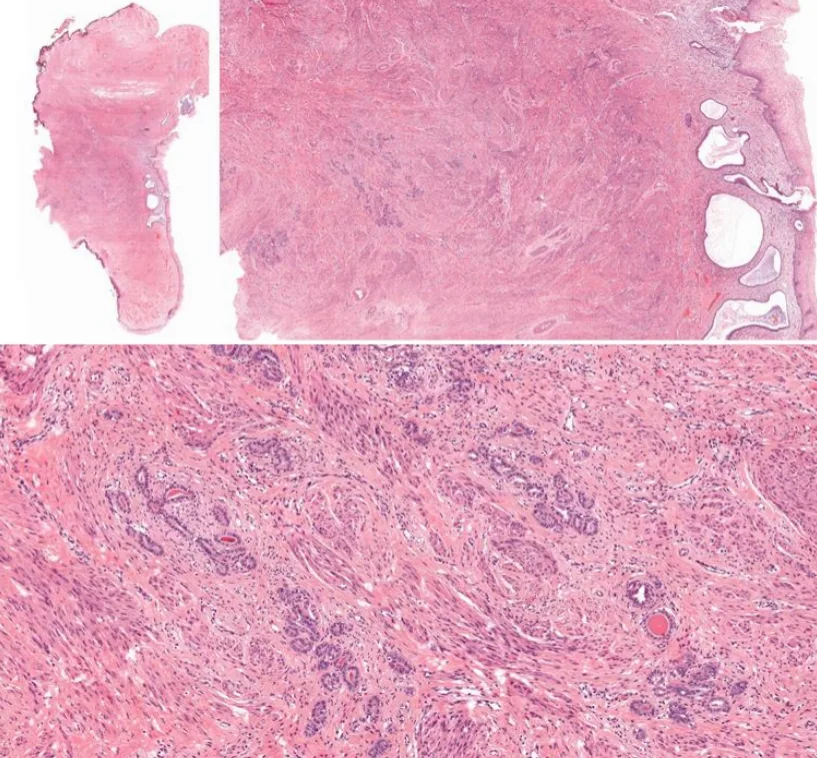
16 y.o, female, abdominal mass, left ovary, high serum calcium. One representative section.
Educational notes:
1. The left ovarian mass is composed of diffuse growth of small cells showing irregular round to oval nuclei with small nucleoli. The cytoplasm is scanty. Mitoses are scattered. At focal areas, cystic spaces containing light eosinophilic secretion is observed.
These small cells are focally immunoreactive towards CKMNF116, CD10, calretinin, EMA, and synaptophysin.
They are diffusely positive for WT1.
They are negative for chromogranin and inhibin.
2. Morphologically, the ovarian mass is composed of undifferentiated small cells with a high mitotic count. Small cell carcinoma of hypercalcemic type of the ovary (SCCHT) and granulosa cell tumor of the juvenile type (JGCT) are the main differential diagnoses in this young female patient.
3. In JGCT, follicle-like spaces containing eosinophilic or basophilic secretions are more numerous. JGCT may have fibrous septa and fibrothecomatous component. In contrast, SCCHT has focal follicle-like spaces with scanty stroma. The most useful immunohistochemical marker to differentiate between these two is inhibin whereby it is positive in JGCT but negative in SCCHT.
4. Clinically, SCCHT is usually associated with hypercalcemia whereas JGCT with estrogenic manifestations.
5. JGCT mostly presents at stage I with excellent prognosis whereas SCCHT is a highly aggressive tumor with a poor prognosis (almost all patients with a stage higher than stage Ia died of disease)
Reference
1. Soslow, R. A., & Tornos, C. (Eds.). (2011). Diagnostic pathology of ovarian tumors. Springer Science &
Business Media.
2. Kurman, R. J., Carcangiu, M. L., Herrington, C. S., & Young, R. H. (2014). WHO classification of tumours of
female reproductive organs. Lyon: International Agency for Research on Cancer.
1. The left ovarian mass is composed of diffuse growth of small cells showing irregular round to oval nuclei with small nucleoli. The cytoplasm is scanty. Mitoses are scattered. At focal areas, cystic spaces containing light eosinophilic secretion is observed.
These small cells are focally immunoreactive towards CKMNF116, CD10, calretinin, EMA, and synaptophysin.
They are diffusely positive for WT1.
They are negative for chromogranin and inhibin.
2. Morphologically, the ovarian mass is composed of undifferentiated small cells with a high mitotic count. Small cell carcinoma of hypercalcemic type of the ovary (SCCHT) and granulosa cell tumor of the juvenile type (JGCT) are the main differential diagnoses in this young female patient.
3. In JGCT, follicle-like spaces containing eosinophilic or basophilic secretions are more numerous. JGCT may have fibrous septa and fibrothecomatous component. In contrast, SCCHT has focal follicle-like spaces with scanty stroma. The most useful immunohistochemical marker to differentiate between these two is inhibin whereby it is positive in JGCT but negative in SCCHT.
4. Clinically, SCCHT is usually associated with hypercalcemia whereas JGCT with estrogenic manifestations.
5. JGCT mostly presents at stage I with excellent prognosis whereas SCCHT is a highly aggressive tumor with a poor prognosis (almost all patients with a stage higher than stage Ia died of disease)
Reference
1. Soslow, R. A., & Tornos, C. (Eds.). (2011). Diagnostic pathology of ovarian tumors. Springer Science &
Business Media.
2. Kurman, R. J., Carcangiu, M. L., Herrington, C. S., & Young, R. H. (2014). WHO classification of tumours of
female reproductive organs. Lyon: International Agency for Research on Cancer.
0 Comments