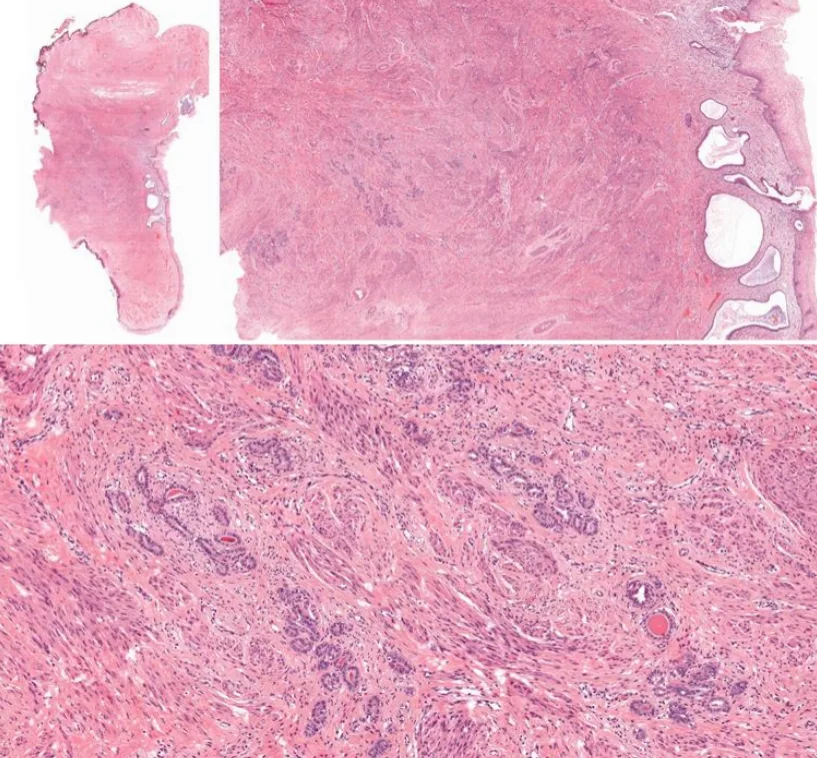
Case 9 - A 46 y.o. LADY
was diagnosed with adenocarcinoma in situ on pap smear and she underwent cervical cone biopsy. One representative section.
🎯𝘛𝘈𝘙𝘎𝘌𝘛𝘌𝘋 𝘋𝘐𝘈𝘎𝘕𝘖𝘚𝘐𝘚 🎯
- Published on
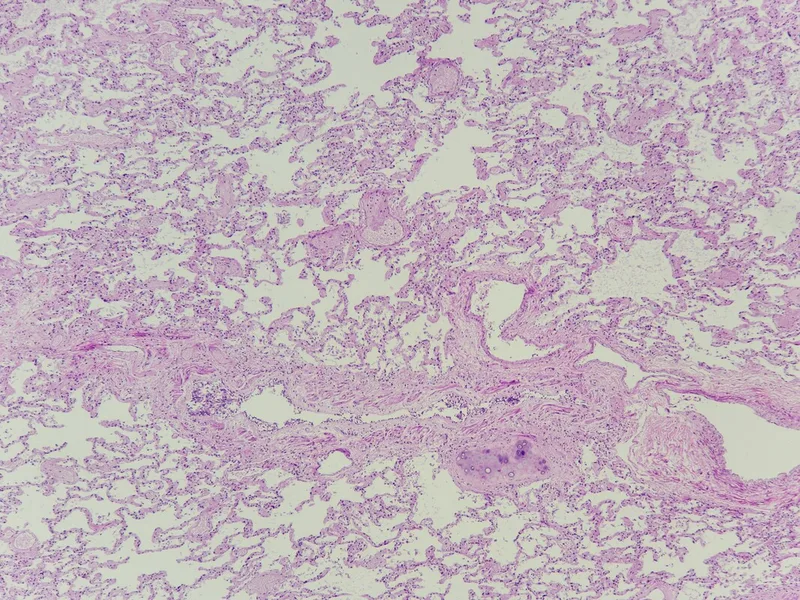
Case 2 - 43 years old lady with severe dengue. Incidental finding during postmortem: Right upper lobe lung nodule.
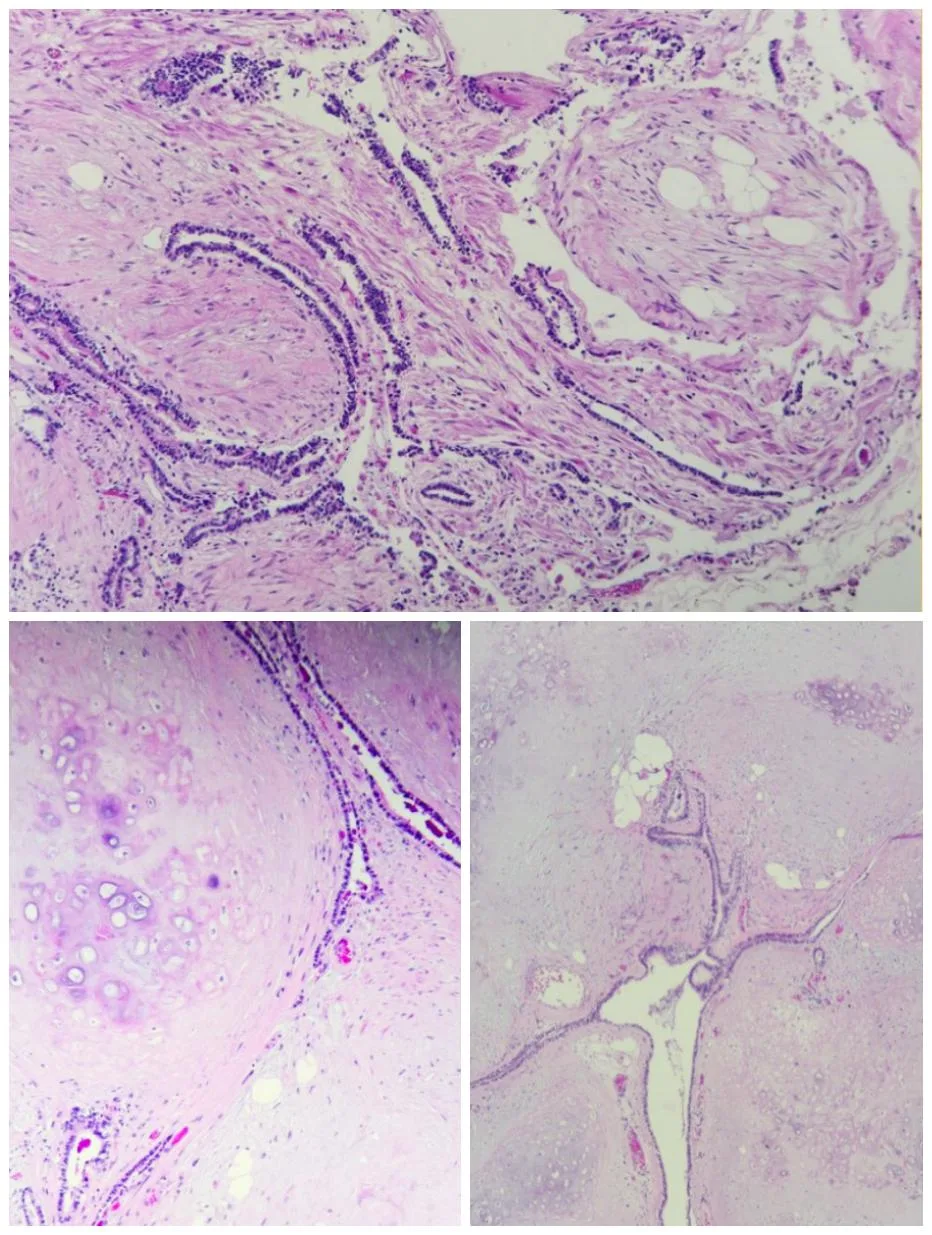
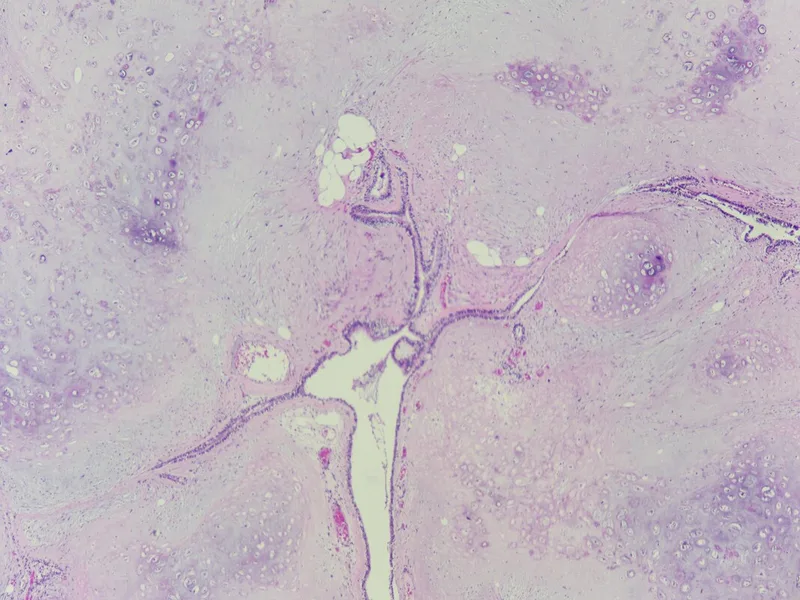
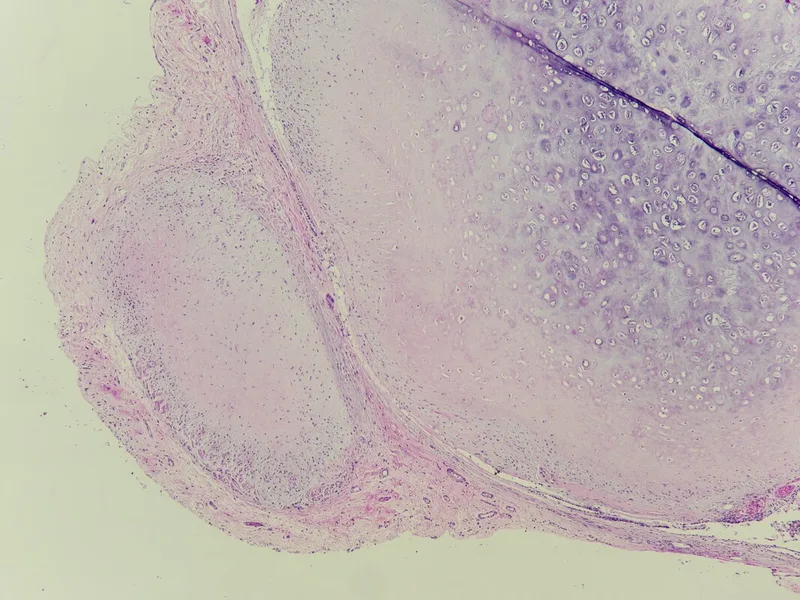
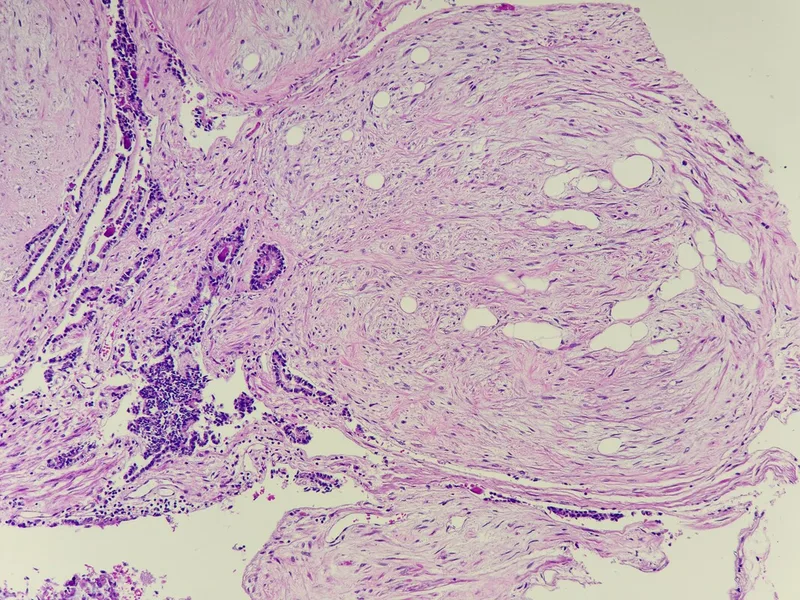
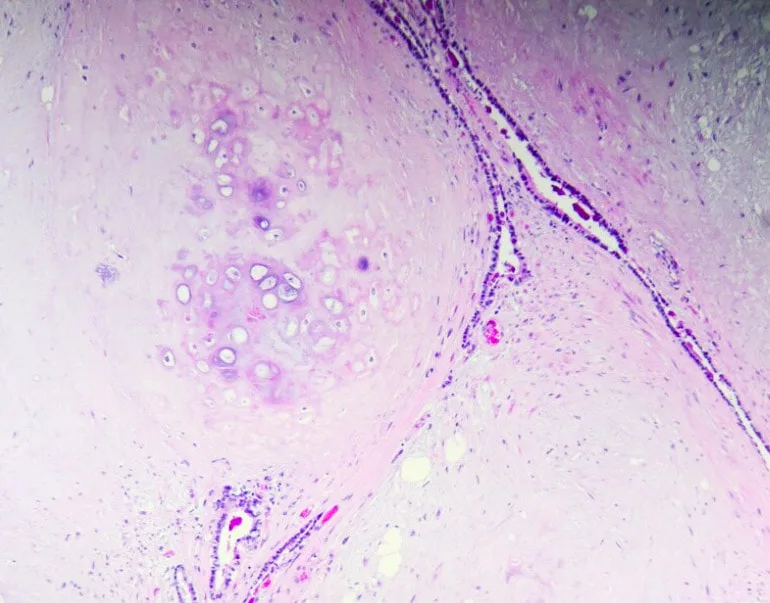
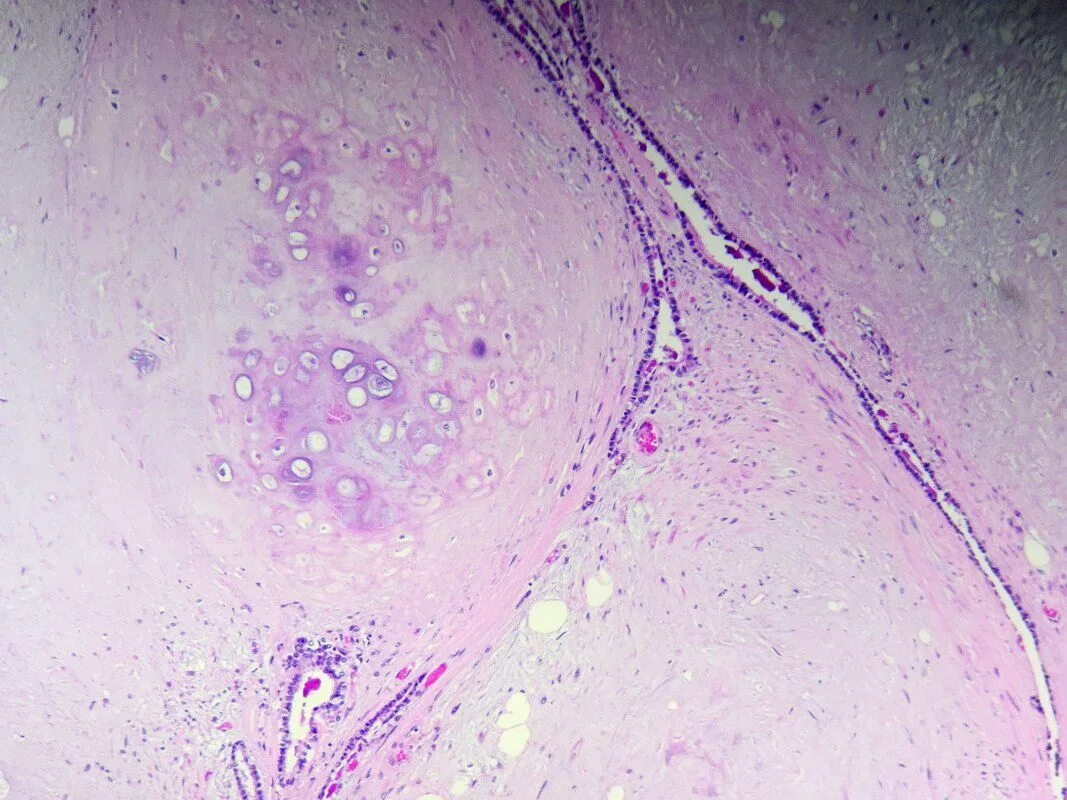
Histopathology of pulmonary hamartoma:
* Gross appearance: Pulmonary hamartomas are typically well-circumscribed, solitary nodules that can range in size from a few millimeters to several centimeters (Most are less than 40 mm) . They often have a firm, rubbery texture and may have a gritty or calcified feel due to the presence of cartilage.
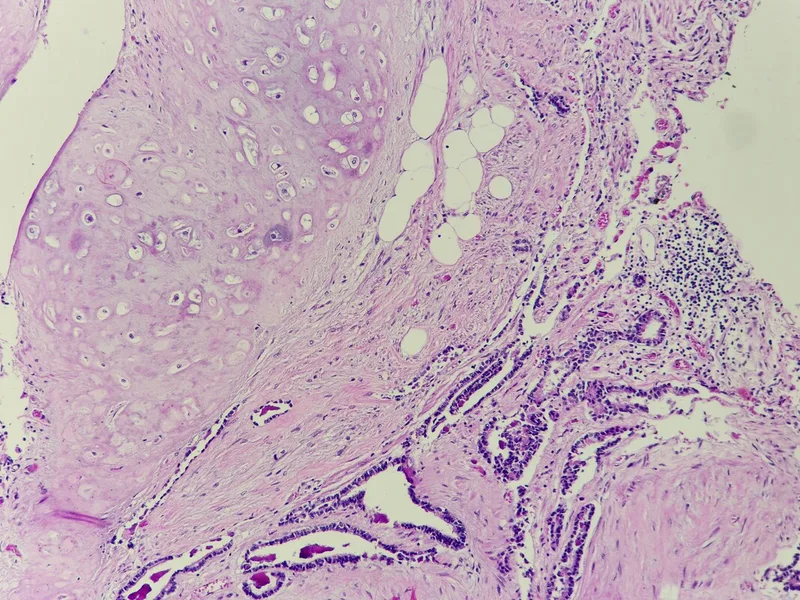
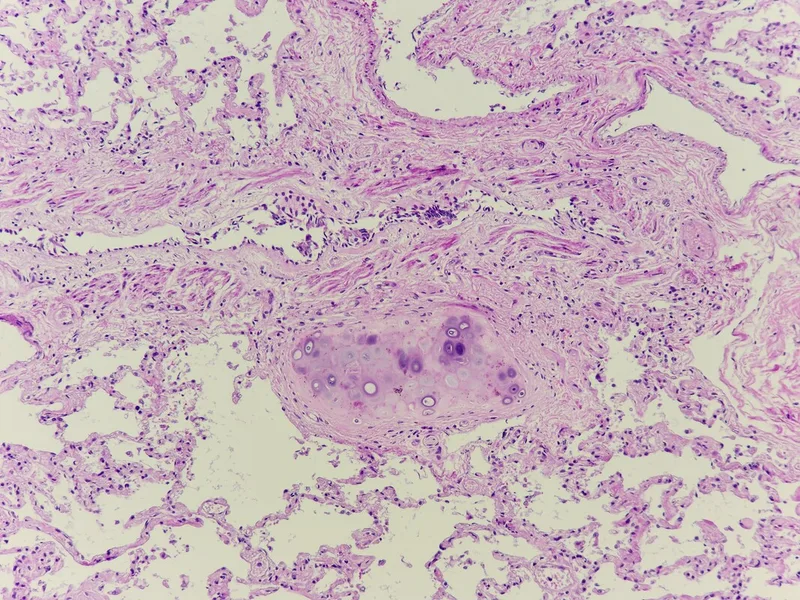
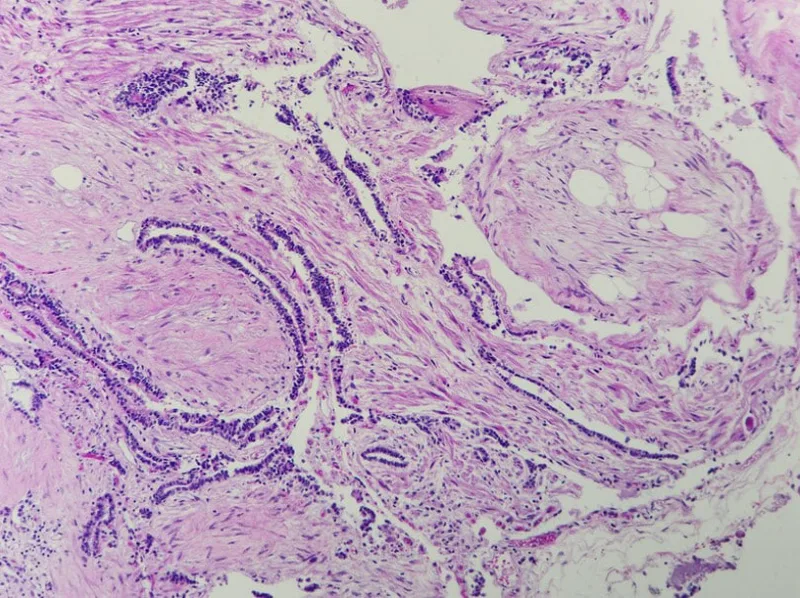
* Microscopic appearance: Histologically, pulmonary hamartomas are characterized by a haphazard arrangement of mature mesenchymal elements, such as cartilage, fat, bland myxoid spindle cells, smooth muscle, fibrous connective tissue and bone, interspersed with islands of respiratory epithelium. The cartilage is often hyaline or fibrocartilaginous and may show calcification or ossification. The fat cells are mature adipocytes. The smooth muscle cells are arranged in bundles or sheets. The respiratory epithelium is typically normal and may line cysts or alveolar spaces.
Key features for diagnosis:
* Presence of at least two different benign mesenchymal elements (e.g., cartilage and fat, cartilage and smooth muscle, or fat and myxoid spindle cells)
* Entrapment of respiratory epithelium within the mesenchymal elements
Additional notes:
* Pulmonary hamartomas are usually benign and do not require treatment unless they are causing symptoms or are large enough to be mistaken for a malignancy.
* In rare cases, pulmonary hamartomas may be associated with other conditions, such as Carney triad, which is a syndrome that includes pulmonary hamartoma, functioning extra-adrenal paragangliomas, and gastrointestinal stromal tumors.
Differential diagnosis :
* Monomorphic soft tissue tumours - Presence of more than one mesenchymal component in pulmonary hamartoma.
* Pulmonary chondromas - Typically arise in patients with Carney triad and lack entrapped epithelium. SDHB immmunohistochemistry may be useful; it shows abnormal loss in Carney-associated chondroma , but not in pulmonary hamartoma.
* Endobronchial lipoma Vs lipomatous hamartoma, whereas epithelial inclusions tend to be inconspicuous- Distinction is generally not critical.
* If only myxoid spindle cell component is sampled - which could lead to consideration of myxoid periheral nerve sheath tumour or even myxoid sarcoma - Unlike those of sarcomas, the spindle cells of hamartoma are generally very bland, without atypia, and they have very low cellularity.
* Monomorphic soft tissue tumours - Presence of more than one mesenchymal component in pulmonary hamartoma.
* Pulmonary chondromas - Typically arise in patients with Carney triad and lack entrapped epithelium. SDHB immmunohistochemistry may be useful; it shows abnormal loss in Carney-associated chondroma , but not in pulmonary hamartoma.
* Endobronchial lipoma Vs lipomatous hamartoma, whereas epithelial inclusions tend to be inconspicuous- Distinction is generally not critical.
* If only myxoid spindle cell component is sampled - which could lead to consideration of myxoid periheral nerve sheath tumour or even myxoid sarcoma - Unlike those of sarcomas, the spindle cells of hamartoma are generally very bland, without atypia, and they have very low cellularity.
Pulmonary hamartoma is a benign (non-cancerous) tumor that develops in the lung. It's actually the most common type of benign lung tumor, accounting for about 8% of all lung tumors and 6% of solitary pulmonary nodules (lumps in the lung). Here's what you need to know about pulmonary hamartoma:
What is a pulmonary hamartoma?
* A hamartoma is a type of benign tumor that grows slowly and is made up of different types of tissue, such as cartilage, fat, connective tissue, and smooth muscle.
* It's considered a hamartoma because it contains disorganized but mature tissues that are normally found in the lung.
* Pulmonary hamartomas are usually small and slow-growing, and they don't spread to other parts of the body (metastasize).
* Molecular and cytogenetic data suggest a neoplastic origin, with recurrent tranlocations leading to fusion genes that drive tumorigenesis.
What are the symptoms of pulmonary hamartoma?
* Most peripheral pulmonary hamartomas don't cause any symptoms and are found incidentally on a chest X-ray or CT scan done for another reason.
* However, if the hamartoma is large or located in the central part of the lung (Endobronchial hamartomas) , it may cause symptoms such as:
* Cough
* Shortness of breath
* Chest pain
* Hemoptysis (coughing up blood)
How is pulmonary hamartoma diagnosed?
* Chest X-ray: This is often the first test done to detect a lung nodule. It may show a well-defined, round or oval nodule with a popcorn-like calcification (calcium deposits).
* CT scan: This provides a more detailed image of the lung and can help confirm the diagnosis of hamartoma. It may show a nodule with a characteristic "popcorn" appearance due to the calcification.
* Localization : Most are peripheral, with approximately 10% located centrally in a bronchus. Hamartomas occur in all lobes. Multifocality is rare.
* Sometimes, a biopsy may be needed to confirm the diagnosis. This can be done by bronchoscopy (a thin tube with a camera is inserted into the lung) or by surgery to remove the nodule.
What is the treatment for pulmonary hamartoma?
* Most pulmonary hamartomas don't require treatment, especially if they're small and asymptomatic.
* However, if the hamartoma is causing symptoms or is large, surgery may be recommended to remove it.
* Surgical resection is also the optimal treatment for endobronchial lesions.
* The type of surgery will depend on the size and location of the hamartoma. Small hamartomas can often be removed with a minimally invasive procedure called video-assisted thoracoscopic surgery (VATS). Larger hamartomas may require open-chest surgery.
What is the prognosis for pulmonary hamartoma?
The prognosis for pulmonary hamartoma is excellent. Once the hamartoma is removed, the cure rate is almost 100%. Recurrence and malignant transformation are very rare.
Reference : WHO classification of tumours - Thoracic tumours (5th Ed.)
* Most pulmonary hamartomas don't require treatment, especially if they're small and asymptomatic.
* However, if the hamartoma is causing symptoms or is large, surgery may be recommended to remove it.
* Surgical resection is also the optimal treatment for endobronchial lesions.
* The type of surgery will depend on the size and location of the hamartoma. Small hamartomas can often be removed with a minimally invasive procedure called video-assisted thoracoscopic surgery (VATS). Larger hamartomas may require open-chest surgery.
What is the prognosis for pulmonary hamartoma?
The prognosis for pulmonary hamartoma is excellent. Once the hamartoma is removed, the cure rate is almost 100%. Recurrence and malignant transformation are very rare.
Reference : WHO classification of tumours - Thoracic tumours (5th Ed.)
0 Comments