Case 9 - A 46 y.o. LADY
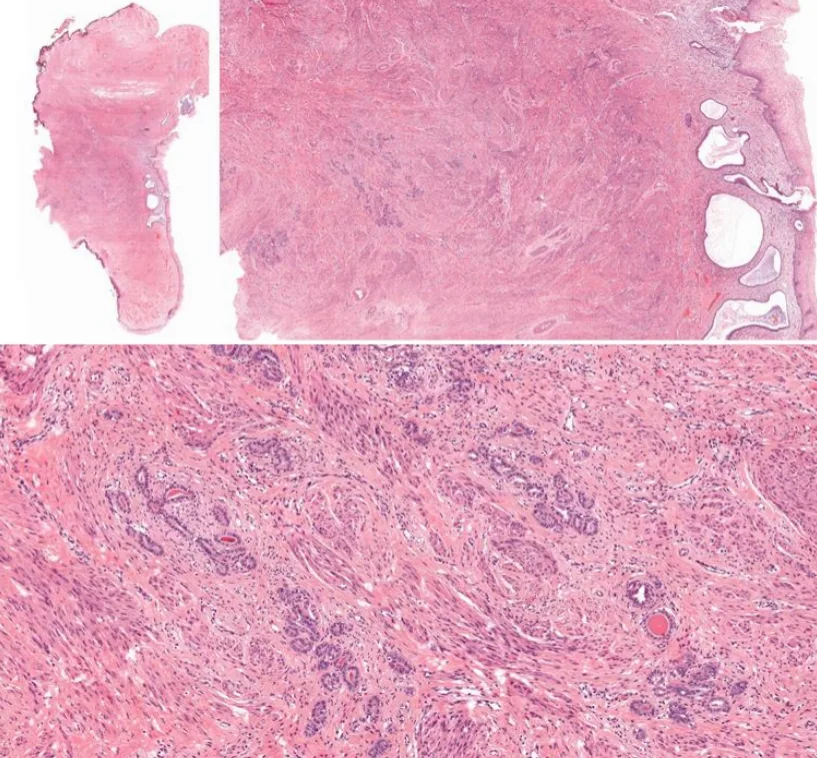
was diagnosed with adenocarcinoma in situ on pap smear and she underwent cervical cone biopsy. One representative section.
🎯𝘛𝘈𝘙𝘎𝘌𝘛𝘌𝘋 𝘋𝘐𝘈𝘎𝘕𝘖𝘚𝘐𝘚 🎯
- Published on
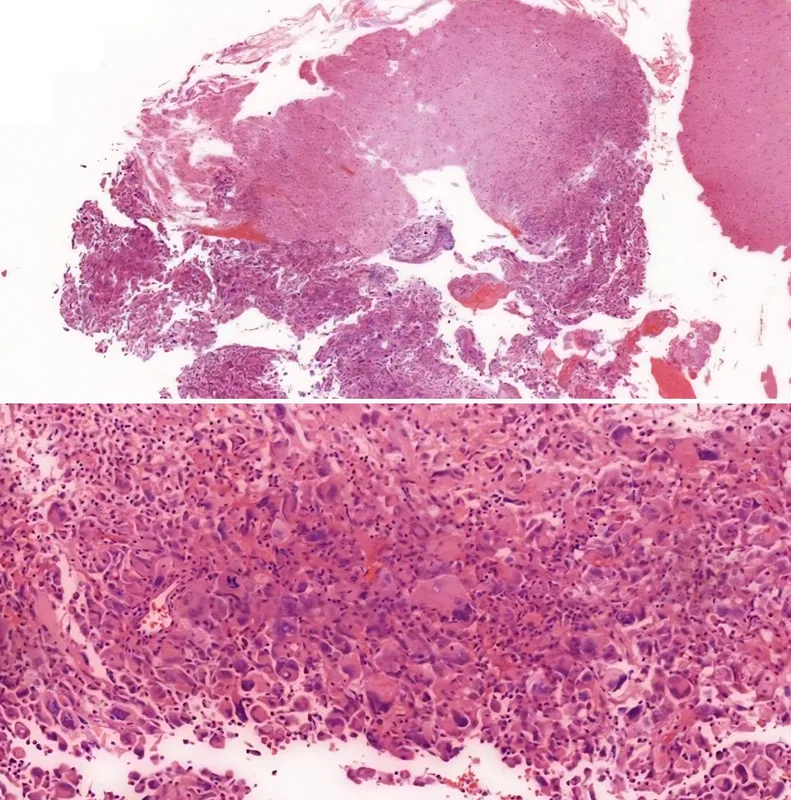
32 y.o., female, multiple hyperdense lesions on the right parietal region. One representative section.Immunohistochemistry shows the malignant cells are positive for GFAP and negative for pan-cytokeratin and HMB-45.
Educational notes:
1. Section shows tumor tissue fragments composed of bizarre malignant cells with angulated hyperchromatic nuclei and abundant cytoplasm. Numerous multinucleated tumor giant cells are admixed. Mitoses are easily observed. The adjacent glial tissue is focally infiltrated by malignant
cells. Immunohistochemistry shows the malignant cells are positive for GFAP and negative for pan-cytokeratin and HMB-45. Histological findings are consistent with giant cell glioblastoma, WHO grade IV. (Note: Without IDH evaluation, a diagnosis of glioblastoma, NOS, is more appropriate, vide infra)
2. The 2016 World Health Organization Classification of Tumors of the Central Nervous System employs integrated phenotypic and genotypic parameters for tumor classification. Glioblastomas are classified into (1) glioblastoma, IDH-wildtype (about 90 %), which corresponds to the clinically defined primary or de novo glioblastoma in older patients; (2) glioblastoma, IDH-mutant (about 10%), which corresponds to secondary glioblastoma with a history of prior lower grade diffuse glioma in younger patients, and (3) glioblastoma, NOS, a diagnosis for those tumors that IDH
evaluation cannot be performed.
3. Along with gliosarcoma and epithelioid glioblastoma, giant cell glioblastoma is a variant under the umbrella of glioblastoma, IDH-wildtype. Histologically, it is characterized by bizarre, multinucleated giant cells and an occasionally abundant reticulin network. Palisading and large
ischaemic necroses are observed. Atypical mitoses are frequent. Microvascular proliferation is not common. Giant cell glioblastoma has a somewhat better prognosis than ordinary glioblastoma.
Reference:
1. World Health Organization. (2016). WHO Classification of Tumours of the Central Nervous System Revised 4th Edition. David N. Louis, (Ed.). Internat. Agency for Research on Cancer.
1. Section shows tumor tissue fragments composed of bizarre malignant cells with angulated hyperchromatic nuclei and abundant cytoplasm. Numerous multinucleated tumor giant cells are admixed. Mitoses are easily observed. The adjacent glial tissue is focally infiltrated by malignant
cells. Immunohistochemistry shows the malignant cells are positive for GFAP and negative for pan-cytokeratin and HMB-45. Histological findings are consistent with giant cell glioblastoma, WHO grade IV. (Note: Without IDH evaluation, a diagnosis of glioblastoma, NOS, is more appropriate, vide infra)
2. The 2016 World Health Organization Classification of Tumors of the Central Nervous System employs integrated phenotypic and genotypic parameters for tumor classification. Glioblastomas are classified into (1) glioblastoma, IDH-wildtype (about 90 %), which corresponds to the clinically defined primary or de novo glioblastoma in older patients; (2) glioblastoma, IDH-mutant (about 10%), which corresponds to secondary glioblastoma with a history of prior lower grade diffuse glioma in younger patients, and (3) glioblastoma, NOS, a diagnosis for those tumors that IDH
evaluation cannot be performed.
3. Along with gliosarcoma and epithelioid glioblastoma, giant cell glioblastoma is a variant under the umbrella of glioblastoma, IDH-wildtype. Histologically, it is characterized by bizarre, multinucleated giant cells and an occasionally abundant reticulin network. Palisading and large
ischaemic necroses are observed. Atypical mitoses are frequent. Microvascular proliferation is not common. Giant cell glioblastoma has a somewhat better prognosis than ordinary glioblastoma.
Reference:
1. World Health Organization. (2016). WHO Classification of Tumours of the Central Nervous System Revised 4th Edition. David N. Louis, (Ed.). Internat. Agency for Research on Cancer.
0 Comments